
Mental Illness Among Refugees in the Middle East




By Alyssa Clark, Will Hayden, and Chloe Jensen
Published Winter 2018
Special thanks to Marissa Getts for editing and research contributions
+ Summary
Refugees are particularly susceptible to mental illness because of the situations they are forced to flee and the uncertainty they face in new countries. Mental illnesses can keep refugees from living high-quality lives. Refugees, particularly in the Middle East, face many barriers to receiving treatment for mental illness. Destigmatizing mental illness and providing access to high-quality, culturally appropriate mental health care are key practices in treating mental illness among refugees.
+ Key Takeaways
+ Key Terms
Depression—“A common but serious mood disorder” officially known as Major Depressive Disorder.1 It causes feelings of sadness, can lead to a lack of interest in activities once enjoyed, and presents a variety of other physical or emotional symptoms.2
Internally displaced people (IDP)—Persons who have not crossed an international border but have been forced to flee from their homes because of conflict. International laws do not protect these people because they have not crossed into another country and thus do not qualify for the same rights and protections as refugees.3
Inter-Agency Standing Committee (IASC)—A committee created in 1992 by the United Nations for coordination between various humanitarian organizations in response to complex emergencies and natural disasters.4
Mental health—“A state of well-being in which an individual realizes his or her own abilities, can cope with the normal stresses of life, can work productively, and is able to make a contribution to his or her community.”5
Post-traumatic stress disorder (PTSD)—“A disorder that develops in some people who have experienced a shocking, scary, or dangerous event.”6
Refugee—A person who has fled his or her home country and crossed an international border because of conflict or persecution for reasons of race, religion, nationality, social group membership, or political opinion. Refugees are recognized as needing international protection.7
Stigma—“A set of negative and often unfair beliefs that a society or group of people have about something.”8 To stigmatize someone is to treat someone unfairly based on a set of negative beliefs about the person. Mentally ill people worldwide are often stigmatized because of their illnesses.9, 10
Context
Mental health refers to a person's psychological or emotional condition. Mental health issues are more than just feeling sad or worried; they are real disorders diagnosed by health professionals that affect many aspects of a person's life, like how the person thinks, feels, and even acts.11 Mental illnesses are typically a result of chemical imbalances in the brain, genetic factors, or a reaction to environmental stressors.12
For a healthcare professional to diagnose a person with a mental disorder, the person must show evidence of several specific changes in behavior or a high level of suffering from a specific symptom.13 Indicators can be categorized
- emotionally (for example, sadness, grief, or fear);
- cognitively (for example, loss of control, helplessness, or worry);
- physically (for example, fatigue, problems sleeping, or loss of appetite); and
- socially/behaviorally (for example, withdrawal or aggression).14
The World Health Organization (WHO) outlines specific pressures that can compromise one's mental health: rapid social change, risks of violence, and human rights violations, among others.15 War and conflict cause many of the pressures that can affect a refugee’s mental health. Trauma from conflict is likely the main reason refugees suffer from mental health disorders at higher rates than the general population.16
Refugees often witness the horrific events that cause their displacement. After fleeing their homes, they are typically left with unstable living conditions and limited economic opportunity.17 These conditions contribute to poor mental health. Refugees increase their risk of developing mental illness increases when they do not have a secure environment and when their physical needs are not met.18
Refugees are much more likely to suffer from mental illness than non-refugees.19 The most accurate studies show that between 13% and 25% of the world's refugees show symptoms of post-traumatic stress disorder (PTSD) (By comparison, the PTSD rates for the general American population are estimated to be 3%—6%).20,21 This trend holds true among refugee populations in the Middle East. One source states that about 41% of Syrian refugees have some form of mental illness,22 compared to only about 17.5%—27% of people in China,23 Europe,24 or the United States who have mental illness.25 Among Palestinian refugees in Lebanon's Burj el-Barajneh camp in 2011, over 70% of Medecins Sans Frontieres (MSF) patients had symptoms of mental illness.26 In short, mental illness rates are consistently higher among refugee populations.
As of June 2017, there were 65.6 million forcibly displaced people worldwide.27 Of these people, 22.5 million are registered as refugees, over half of whom are younger than 18 years old.28 There are also many millions of internally displaced people (IDPs). Fifty-five percent of the world's refugees come from three countries: Syria, Afghanistan, and Sudan.29 There were 5.5 million Syrian refugees and 2.5 million Afghan refugees as of June 2017.30 Ten percent of Iraq's population, or 3.4 million people, have been displaced.31
Refugees in the Middle East come from diverse social, socioeconomic, ethnic, and religious backgrounds. The refugee population is also linguistically diverse: the Middle East is home to a host of languages, including (but not limited to) Arabic, Persian, Hebrew, Turkish, Kurdish, Turkmen, Armenian, Syriac, and Socotri.32 Although many refugees from the Middle East are Muslim, others are Christian, Jewish, Bahaist, Druze, or Hindu.33, 34 Finally, differences in age and gender also diversify the population.35
Within refugee populations, some groups are particularly vulnerable to mental illness. These vulnerable groups include the following:
- The elderly: a study in Lebanon showed that compared to other refugees, elderly refugees were three times as likely to show symptoms of mental illness.36
- Children: nearly 50% of Syrian refugee children suffer from PTSD.37
- Victims of torture: in general, survivors of torture are at higher risk of developing mental illnesses than the general population.38 As of March 2018, there appears to be no data on the percentage of refugees who have experienced torture.
- Victims of sexual or gender-based violence: conflict and displacement lead to an increase in both forms of violence, as well as an increase in the incidence of early marriage.39 These increases contribute to the stress, fear, and stigma associated with poor mental health.40
- LGBTI (lesbian, gay, bisexual, transgender, and intersex) individuals: unique stressors, including extreme stigma and vulnerability to abuse, affect these individuals, and these stressors can contribute to poor mental health.41 As of March 2018, there appears to be no data on the percentage of refugees who experience stigma due to sexual orientation.
Contributing Factors
Trauma
Traumatic experiences contribute to mental health issues among refugees. Refugees and IDPs often witness and experience conflict-related violence, including torture, rape and sexual violence, murder, massacres, and daily violence such as bombing and shelling.42 Such violence causes refugees to flee their homes. The routes refugees take are not always safe; one Syrian road is nicknamed the Death Road because it is so dangerous.43 For many refugees, even refugee camps are places where violence and insecurity are the norm.44
The prevalence rates of torture, rape, death, and other trauma experienced in the refugees' home countries vary but increase with conflict. As an example, 13% of Syrian refugees have lost a family member in the country's civil unrest, and two-thirds of Syrian refugees had their homes damaged or destroyed.45 Rape and gender-based violence rates in the Middle East have risen since 2011;46 some soldiers in Middle East conflicts report being ordered to rape.47 Prevalence is difficult to estimate for two reasons: the stigma of sexual violence and the lack of access human rights workers have to conflict areas.48 Despite these limitations, qualitative research suggests many refugees are raped and do not report it.49 Torture prevalence rates are also inexact for similar reasons.
Research indicates that trauma increases the risk of mental illness. A meta-analysis of over 150 studies on refugee populations found that torture was associated with increased rates of both PTSD and depression.50 The same research suggested that other traumatic experiences were strongly correlated with depression.51
Instability
Refugees and IDPs face daily stressors resulting from poverty, loss of employment, loss of education, and lack of basic needs like housing and food. When refugees lack adequate income, they often turn to survival strategies that damage their health and well-being. These strategies include going into debt, living in illegal housing, working informal jobs with the potential for employer abuse, survival sex/prostitution, and child labor.52
These initial stressors can, in turn, lead to more social stressors like stigmatization or shame. For example, rape victims often face stigmatization, and former breadwinners who can no longer provide for their families experience shame. These social stressors contribute to poor mental health.53
Refugees face serious uncertainty, which contributes to poor mental health. For example, not knowing where loved ones are or whether they are safe causes a great deal of stress.54 Uncertainty or a lack of information about family members, friends, and the state of conflict all increase stress. Studies suggest that refugees in temporary camps and unstable environments face higher rates of PTSD than refugees who are resettled.55
Many refugees live in diverse communities that change regularly. Refugee camps see new arrivals constantly. Such high turnover can disrupt social structures. The significant diversity among refugee populations often results in a lack of cohesion.56 These social factors combine to cause conflicts, violence, and social isolation that contribute to poor mental health.57
Consequences
Mental illness has many long-term, far-reaching effects on individuals and society. There are various symptoms of each illness, and people can experience each illness differently. A person may experience all, none, or some of the negative effects of mental illness. According to the Mayo Clinic, these negative consequences include the following:
- Unhappiness or decreased life enjoyment
- Conflicts in families
- Difficulties with relationships
- Tobacco, alcohol, or drug abuse
- Legal problems
- Financial problems
- Poverty or homelessness
- Social isolation
- Problems at school or work
- Self-harm or violence towards others (including suicide and homicide)
- A weakened immune system, heart disease, and other physical consequences58
Refugees are likely to face many of these challenges (such as financial problems or social isolation) because of the instability that comes with fleeing their home country. In addition, they often face continuing trauma and insecurity after fleeing violence. These difficulties often compound already challenging circumstances and can halt mental health treatment.
Mild mental health problems can become serious if left untreated for an extended period of time.59 Serious cases require more intense treatment and, in some cases, hospitalization. Studies show high rates of PTSD among displaced persons not only during, but also long after conflict. One in five Turkish Cypriots who were internally displaced during Turkey's 1974 invasion of Cyprus still had PTSD nearly three decades later.60 Treating mild cases early may prevent the need for extensive (and expensive) care for chronic or more serious conditions.
Widespread mental health problems impact society as a whole. Mental illness can lead to productivity loss, which, in aggregate, can devastate economies.61 Similarly, because mental illness can increase the risk of violence, populations with many people suffering from mental health issues could face increased interpersonal violence.62
Barriers to Treatment
Culture
Cultural differences add to the difficulty of addressing mental health issues for refugees. Seeking help for mental disorders may be culturally awkward or unacceptable; in some countries, dealing with mental health issues translates to being “crazy.”63 It is often difficult and uncomfortable for refugees to discuss personal losses and emotional difficulties with medical professionals;64 this barrier keeps many from seeking help.65 Additionally, in the cultures of some refugees, mental health is deeply connected to religious belief and supernatural causes; still, in other cultures, mental health problems are not viewed as separate from physical illness.66
Language can also be a major barrier to care for mental illness among refugees. Because refugee communities often comprise individuals whose language differs from the host country's language, refugees often struggle to find mental healthcare resources in their native language. When refugees do overcome the language barrier, they might describe symptoms of their mental health condition in physical or spiritual terms like, “My head is heavy,” or “I no longer have the will,” which may be unfamiliar to Western medical professionals.67
Further, refugees who live among diverse people in camps or urban areas may lack a sense of community. Many refugees live in fairly transient communities, where people are constantly entering and leaving. Since community and social support is an important aspect of coping with mental health issues, the diversity in refugee communities may be a potential obstacle to treating mental health issues.
Lack of Resources
There are few psychologists in host countries. Eighty percent of the world's refugees live in low-income countries, which tend to have fewer mental health specialists.68 In Syria, Lebanon, Jordan, and Turkey, where there are many Syrian refugees and IDPs, there are between 1 and 4 psychiatrists per 300,000 people.69 Many refugees, particularly in Jordan, live in urban areas and cannot access the care provided in refugee camps.70
Typically, refugees have many other needs that are prioritized above mental health services. Within forcibly displaced populations, addressing basic needs such as food, shelter, security, winterization, and medical treatment for wounds take priority over mental health care.71 In Jordan, the ratio of medical doctors to psychiatrists is only 1 to 30.72 This scarcity of medical doctors partially explains why most aid organizations prioritize providing physical health care and other aid over mental health care.
Children
Refugee children face unique mental health challenges, which can make diagnosis and treatment difficult. Children mature at different paces as they learn to cope and relate to others.73 Like adults, children need stable environments for proper mental health. One major source of stability for children is education. However, many refugee children do not have access to schools; in Jordan, only 40% of Syrian refugee children attend school.74 Many children have cognitive learning disabilities caused by the trauma they have faced. The prevalence of these disabilities becomes a greater issue because children facing such challenges require more resources in schools and are more likely to drop out or become unemployed.75
Children may not be able to recognize or communicate their developing mental health issues. Children's symptoms can be different from adults' symptoms.76 For example, children with mental health issues may experience headaches or stomach aches rather than the sadness or anxiety frequent in adults with similar conditions.77 The mental health of parents and other family members will affect a child's mental well-being as well.
Practices
Temporary Humanitarian Healthcare Professionals
To address mental illness among refugees, some aid organizations temporarily send volunteers to affected areas during emergency situations. These volunteers can be either medical professionals who receive training in mental health treatment or specialized mental health professionals. Typically aid organizations integrate mental health care into other medical care at already-established refugee health clinics.78 Aid organizations set up hospitals in safe locations wherever possible; one Medecins Sans Frontieres (MSF) hospital was established in a cave in Syria.79 Mental health professionals focus on using simple, plain terms to maximize understanding and to avoid alienating the refugees. Sometimes, because of language issues, they use well-trained, professional interpreters who know mental health terminology. After the emergency or a set time frame, the health professionals leave.
Two of the biggest aid organizations that implement this practice are the International Medical Corps (IMC) and MSF.80 In 2015, MSF opened hospitals in key locations outside Syria in some of the biggest refugee camps, including Zaatari Camp in Jordan.81
Impact
Psychological treatment (counseling or therapy administered by a health professional, sometimes accompanied by prescribed medicine) can help re-establish good mental health, even in severe cases.82 However, little data is available specifying to what degree refugees are impacted by psychological treatment. Because refugees have so many needs that take priority over data collection, sufficient impact data has yet to be gathered. Further, mental health outcomes are linked to so many factors (environment, time since trauma, current stressors, and so on) that pinpointing the impact of specific interventions is difficult. In terms of service delivery, MSF and IMC's model of working through health clinics delivers moderate amounts of counseling sessions where they operate. In MSF hospitals in Jordan in 2015, over 5,400 psychosocial or counseling sessions were performed,83 and in 2014, over 6,900 mental health consultations were conducted in Iraq.84
Gaps
- Humanitarian responders are temporary and mental health issues are likely to continue and increase as violence continues. While helpful for short-term interventions, humanitarian responders are not a sustainable solution.
- A shortage of mental health professionals among the humanitarian responders often causes delays in care or lower quality care.85
- Refugees are often legally barred from using national health facilities, so aid organizations work parallel to, rather than in tandem with, national governments. This structure creates tension between refugees and their host nations and limits sustainability.86
- Few professional interpreters are familiar with mental health terminology in the various languages refugees speak.
- Informal or non-professional interpreters may be unfamiliar with some terminology, may be part of the same social group as the refugee (creating privacy concerns), or may be refugees themselves, potentially leading to greater stress on their part.87
Training of Trainers Programs
In training of trainers programs, humanitarian organizations instruct local healthcare professionals in mental health treatment, with a focus on counseling. The local professionals then teach other local healthcare professionals to treat mental illness. Trained local professionals are supervised by mental healthcare professionals assigned by the government or the organization running the program to ensure quality of care. The goals of training local persons are as follows:
- Decrease language barriers when local health professionals speak the relevant language.
- Increase the total number of qualified caregivers.
- Increase the number of caregivers available for longer-term care.
Both MSF and IMC use “training of trainers” programs.88, 89/sup> The WHO also works with local doctors to train them on identifying and treating mental health issues.90
A variation of this practice is training people who are not healthcare professionals to treat mental illness. A small group called Syria Bright Future (SBF), founded by a Syrian psychiatrist and refugee in Jordan, takes on community volunteers to assist in mental health care. This training includes recognizing signs and symptoms of mental illness, developing communication skills, and providing first aid for mental illness (initial interventions that can include speaking in a calming voice, facilitating deep breathing, and listening respectfully).91, 92 These volunteers primarily refer people who show signs of mental disorders to the appropriate providers (psychiatrists, psychologists, and other mental health professionals).
Impact
Using a self-report tool endorsed by the WHO, MSF tested 3,800 refugees in Iraq for symptoms of mental illness before and after counseling.93 Ninety-seven percent of those who came to MSF for counseling had significant psychological symptoms at the beginning; this number dropped to 29% by the last counseling session.94
Research suggests that providers who understand the refugees’ culture or language are better able to educate refugees about mental health and mental health care.95 According to a report coauthored by the founder of SBF, families feel safe working with the organization because the health professionals come from the same areas or cities.96
Gaps
- In many Middle Eastern nations, it is difficult to obtain licensure as a mental health professional. In Syria, for example, there is no licensing framework for the field.97 This lack of framework means that there is no way to assess credentials and underqualified individuals could perform care.
- Training of trainers programs work parallel to, rather than in conjunction with the government training and licensure practices currently in place.
- When humanitarian responders leave, the lack of supervision can lead to decreased quality of care.
Structured Recreation
One of the best coping strategies, especially for children, is to engage in structured recreational activities. Recreation is used as therapy all over the world, including at hospitals for mental health. Through recreation, people can relieve stress and form social bonds that help them deal with trauma. This practice targets children because other practices tend to be less effective for children.
Several organizations use recreation for addressing mental health:
- In the Azraq refugee camp in Jordan, IMC created an adolescent-friendly space, which allowed refugee youth to play together as they would under normal conditions.98
- IMC also offers activities for all ages that include cooking, dancing, community events, and English or computer classes.99
- The Sankari Humanitarian Foundation established a center for refugees in Gaziantep, Turkey, that focuses on recreational activities for children.100 The center offers martial arts classes, mosaic-making workshops, astronomy classes, and other recreational opportunities aimed at making children happier.101
Some programs combine recreational activities and mental health education; for example, for one program children watched puppet shows developed in part by a psychiatrist. During this activity, the mothers were gathered and discussed depression (including how to recognize symptoms in children) with psychologists.102
Impact
Research suggests that recreational activities are beneficial to mental health.103 Refugee children need safe places, structured activities, and people who are trained to work with them.104 Safe places provide a space where those who have lost friends can build friendships again.105 Because there are so many variations of the practice, levels of impact may vary.
De-Stigmatization Campaigns
Campaigns to destigmatize mental illness among refugees take many different forms. Effective campaigns are mindful of the cultural stigmas that surround mental health issues and take action to ensure that treatment is accessible to as many people as possible. In 2016, the International Medical Corps (IMC) published a series of educational booklets and distributed them to refugees. These booklets present information on the most common mental health issues in a culture-specific, relatable way. With the booklets, IMC intended to educate people about the signs and symptoms of mental health disorders and to encourage people to seek care.107 IMC also uses the booklets in mental health awareness trainings, in which audiences are tested before and after training to assess understanding. In early 2017, the WHO distributed a similar set of educational materials focusing on depression via local physicians in Turkey and northern Syria.108
Impact
It is generally accepted that increased education and awareness help to decrease stigma.109 As of March 2018, there was little evidence of the direct impact de-stigmatization campaigns have on refugee mental health in the Middle East.
Gaps
- It is nearly impossible to ensure that mental health information reaches every refugee.
- Because stigmas are deep-seated, they may be difficult to overcome even with better awareness.
- Few educational materials seem to target children.
- As with all mental health care, de-stigmatization materials take funding away from other high-priority needs such as food and shelter.
Education
Education, especially for children and youth, serves as a way to re-establish a sense of normality and routine in the lives of refugees. It also provides opportunities to find role models and interact with peers. Students can develop basic life skills that provide cognitive protection during times of distress and conflict.
Education for refugee children is provided in many ways, including refurbishing schools, adding “second shift” classes to deal with the influx of displaced persons, and providing teacher training.110 The International Rescue Committee's approach to education focuses on three areas: helping young children develop cognitive and social-emotional skills, teaching older children literacy and numeracy skills, and helping youth and adults develop skills that will prepare them for the workforce and earn a livelihood.111
The best teacher training programs educate teachers on signs and symptoms so that they can identify at-risk children and direct them to healthcare providers accordingly. Many teachers themselves are displaced, enabling them to act compassionately and empathetically. Additionally, teaching gives adults a purposeful activity after having been displaced by conflict.112 Some schools offer in-school support for students experiencing psychosocial and mental health difficulties. Teacher support groups give teachers an opportunity to get help as needed.113 Providing teachers with support groups minimizes their added stress, helping them prevent mental illness.
Impact
- Aside from research on the benefits of education in the general population, there is little impact data on education and teacher training specific to refugees. Further research is needed to show causal impact.
- UNHCR, in conjunction with Educate A Child (EAC), provided 260,000 refugee children worldwide with access to primary schooling between 2012 and 2015.114 Little data is available about which regions received this aid.
- Research suggests that continued education is one of the most important indicators of a child's well-being.115 Removing physical and emotional stressors removes a risk factor for mental illnesses, so improving overall well-being also helps mental health.
- Education provides youth with the skills and knowledge necessary for higher-paying jobs, thus reducing their chances of working in unskilled labor positions.
- Since preventative practices like education can help prevent mild cases from becoming more severe, they could actually save resources in some cases.
Gaps
- Impact data is needed to show that teacher training helps mental health outcomes in refugee children.
- With so many primary needs (such as food, shelter, and protection) taking priority over secondary needs, such as mental health and education, raising the money needed to provide quality education is challenging. For example, UNHCR received only about 40% of the funds they requested for an education project in 2015.116
- Since funding is required for teacher training, organizations cannot afford to train a sufficient number of teachers on how to identify mental health symptoms in their students.
Cash Assistance
Cash assistance alleviates many of the daily stressors that refugee families face by giving them cash and vouchers to cover the costs of basic needs such as housing, food, and clothing. Recently, aid organizations have also worked with banks to provide funds through ATM cards. Organizations choose individuals and families after assessing household needs and access to resources. The people selected receive an initial cash payment and additional payments thereafter, according to needs and specific circumstances. The UNHCR and IRC are major aid organizations that use cash assistance.

Impact
Cash assistance programs effectively remove stressors such as acute poverty and lack of basic needs, which contribute to mental illness. Measuring how much direct impact cash assistance has on mental health can be difficult. Cash assistance gives refugees a sense of autonomy over their lives and choices, giving them a better sense of stability and normality.117 This increase in control and stability helps refugees to resolve some of the ambiguity that leads to mental illness. In 2014, the IRC conducted an extensive impact evaluation on 87,700 Syrian refugees in Lebanon. The organization first gave each participant $575 USN to help with winterization and then evaluated the outcomes.118 The results showed that cash assistance was useful in meeting basic needs such as food, acting as a multiplier in the Lebanese economy, and combating social ills on a societal level. The social impact included increased education, increased health, decreased household tension, decreased child labor, and decreased tension between refugees and their host country.119 Eighty percent of refugees observed preferred cash assistance to in-kind aid, likely because of increased autonomy.120 Since preventative practices like cash assistance can help prevent mild cases from becoming more severe, they could actually save resources in some cases.
Gaps
- The direct impact of cash assistance on mental health outcomes is difficult to measure.
- Broken economic systems within refugee camps and the corresponding high levels of unemployment make providing for families difficult, even with the aid of cash assistance.
- Organizations struggle to know where to donate money; they must find places with a relatively low risk of inflation and a significant number of displaced people.121
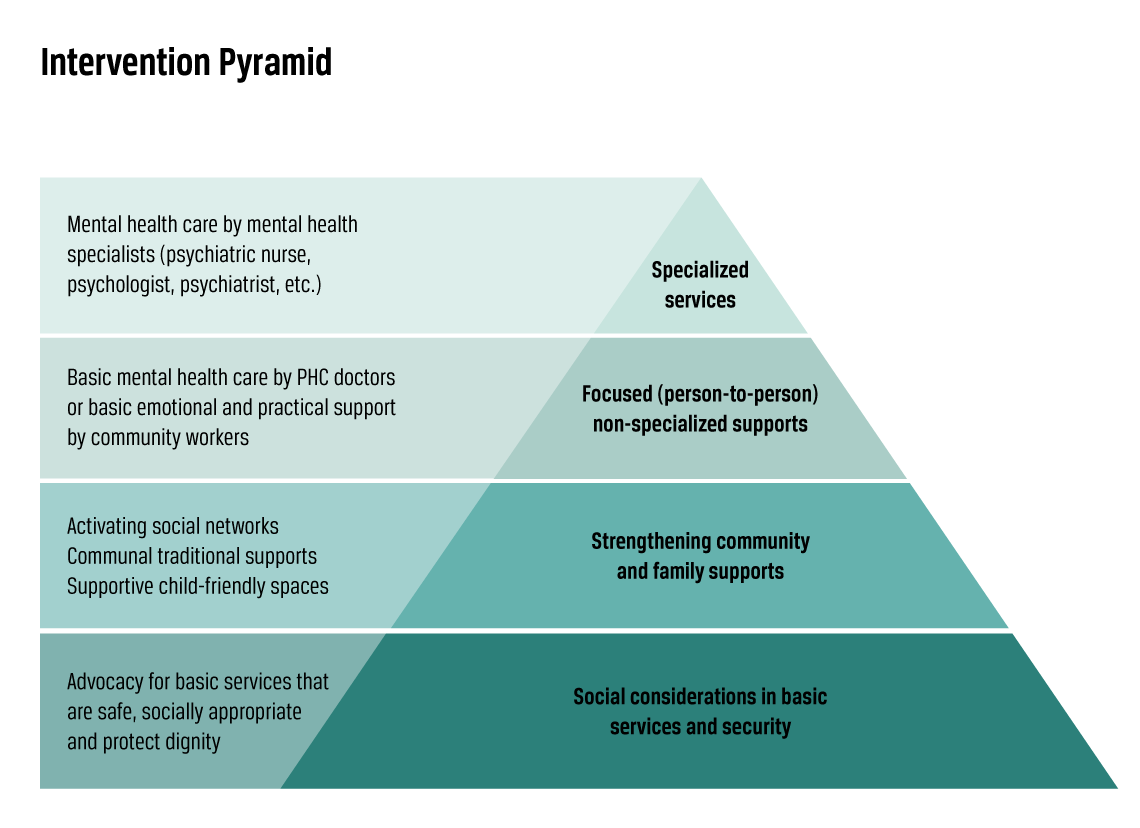
Multilayered Approach
Mental health professionals have begun to call for a multilayered approach to mental health in emergency situations.122 Most practices only deal with one or two layers, though combining and coordinating practices can help achieve the overall aim of the complete intervention pyramid.
Impact
Since this framework is relatively new (introduced in 2007), not many people have fully adopted a multi-tiered approach, and no specific data is available. However, a committee of experts appointed by the WHO recommends that all layers address mental health concerns among refugees fully.
Preferred Citation: Clark, Alyssa, Will Hayden, and Chloe Jensen. “Mental Illness Among Refugees in the Middle East.” Ballard Brief. March 2018. www.ballardbrief.org.
Viewpoints published by Ballard Brief are not necessarily endorsed by BYU or The Church of Jesus Christ of Latter-day Saints