
Prevalence of Alzheimer’s Disease in Adults in the United States

Photo by Andrea Piacquadio


By Margaret George and Erica Bassett
Published Fall 2022
Special thanks to Robyn Mortensen for editing and research contributions
Summary+
Alzheimer's disease (AD) has become increasingly prevalent among adults in the United States, with the CDC estimating that AD affects 5.4 million people in the US. As a neurodegenerative disease, AD leads to life-threatening physical and cognitive effects for adults ages 65 and older. Many risk factors contribute to the possibility of an individual developing AD in the United States. Some of these risk factors an individual can somewhat control, including wellness choices and the quality of one’s social relationships. Other factors are more challenging for an individual to control, such as one’s genetic history and environmental factors like air pollution. The prevalence of AD ultimately results in high mortality and morbidity rates, substantial economic losses, and caregiver burden in the US. Considering that AD currently has no cure, nationwide efforts such as research into wellness programs may help alleviate this issue.
Key Terms+
Alzheimer's Disease (AD)—A degenerative brain disease and the most common form of dementia.1
Alzheimer’s Disease Continuum—The gradual progression of Alzheimer’s Disease from preclinical AD (where no symptoms manifest) to severe dementia (where symptoms interfere with daily living). In the mild stage, most individuals can function independently with difficulty in everyday tasks. In the moderate stage, individuals experience memory and language challenges and may need assistance with tasks like dressing. In the severe stage, individuals require regular care and have significant memory and language challenges. The length of each stage depends on several factors, such as age, sex, and genetics.2, 3
Apolipoprotein-e4 (APOE-e4) Allele—One variation of the Apolipoprotein-e gene, which involves the metabolism and repairing of cell membranes in the central and peripheral nervous systems. This allele most likely contributes to plaque buildup and neurofibrillary tangles, both risk factors for developing Alzheimer’s Disease.4
Atherosclerosis—“The build-up of fats, cholesterol and other substances in and on your artery walls (plaque), which can restrict blood flow.”5
Beta-amyloid Proteins (Aβ protein)—A complex protein found on the surface of cells throughout the body. This protein assists in neural growth and repair. Corrupted forms of this protein destroy neurons and ultimately contribute to Alzheimer’s Disease.6, 7
Chronic Illness—Medical conditions that last one year or more and require ongoing medical attention. Examples of chronic illnesses include arthritis, asthma, diabetes, and heart disease.8
Cortisol—The body’s primary stress hormone. Cortisol increases glucose levels and, when at chronically high levels, can alter the body’s immune system response and increase the risk of various diseases.9
Dementia—“A usually progressive condition (such as Alzheimer's disease) marked by the development of multiple cognitive deficits such as memory impairment, aphasia, and the inability to plan and initiate complex behavior.”10
Disease—“A condition that impairs normal functioning and is typically manifested by distinguishing signs and symptoms.”11
Disorder—“An abnormal physical or mental condition.”12
Gray Matter—Tissue that makes up the outermost layer of the human brain. This brain tissue exists along the brain, brain stem, and spinal cord. Gray matter is dense in unmyelinated axons (creating its pinkish gray tone), whereas white brain matter is composed of myelinated axons. Gray matter contains networks of neurons that are responsible for essential motor functions.13, 14
Morbidity—The condition of ill health or disease.15
Neurofibrillary Tangles—Abnormal accumulations of tau proteins inside neurons, which damages neural networks and prevents the brain from communicating properly. The abnormal accumulations most often reside in brain areas involved in memory.16
Neuroinflammation—An inflammatory response in the brain or spinal cord. While low levels of neuroinflammation can benefit the body’s immune system and brain function, severe neuroinflammation can lead to tissue damage, stress, and cell death.17, 18
Pathology—“The study of the essential nature of diseases and especially of the structural and functional changes produced by them.”19
Resistiveness—Any opposition to care, typically during an encounter between a caregiver and care recipient.20
Risk Factor—“A factor, such as a habit or an environmental condition, that predisposes an individual to develop a particular disease.”21
Tau Protein—A protein that helps stabilize the structure of a neuron and facilitate the transportation of nutrients and other essential molecules. In unhealthy amounts, tau proteins cling to one another instead, creating protein clumps known as neurofibrillary tangles. These neurofibrillary tangles, made up of tau proteins, disrupt neural functions and are a risk factor for AD.22, 23
Context
Q: What is Alzheimer’s, and how does it relate to dementia?
A: Alzheimer’s diseaseA degenerative brain disease and the most common form of dementia.1 (AD) is a neurodegenerative disease“A condition that impairs normal functioning and is typically manifested by distinguishing signs and symptoms.”11 that targets specific brain regions related to memory and executive function. For instance, AD damages the hippocampus and the nearby entorhinal cortex, both involved in forming and storing memories.24 AD also targets the frontal lobe, an area responsible for judgment and behavior, and areas of the cerebral cortex responsible for language, reasoning, and behavior.25 Although AD damages critical brain areas, the disease“A condition that impairs normal functioning and is typically manifested by distinguishing signs and symptoms.”11 does not directly kill an individual. Instead, complications from the decline in brain function lead to death. Some examples of these complications include vascular changes, infections, injuries from falls, and malnutrition.26, 27

Photo by Robina Weermeijer on Unsplash
Although AD manifests itself in various ways, behavioral and cognitive symptoms generally characterize it.28 For example, common cognitive symptoms of AD include forgetfulness, disorientation, confusion, and difficulty staying focused. Individuals with AD may also exhibit behavioral or physical symptoms such as wandering, self-harm, inability to swallow or feed oneself, resistivenessAny opposition to care, typically during an encounter between a caregiver and care recipient.20, and agitation.29 Other general AD symptoms include difficulty staying focused, being increasingly overwhelmed, inability to understand instructions, and difficulty finding the right words.30 Because of these symptoms, individuals with AD often require increased attention or medical care.
A genetic mutation creating excessive production of beta-amyloid proteinsA complex protein found on the surface of cells throughout the body. This protein assists in neural growth and repair. Corrupted forms of this protein destroy neurons and ultimately contribute to Alzheimer’s Disease.6, 7 causes Alzheimer’s diseaseA degenerative brain disease and the most common form of dementia.1. This overproduction of proteins leads to amyloid plaques in blood vessels, which limit blood flow to critical areas of the brain and subsequently destroy brain cells.31, 32 These amyloid plaques are specific to Alzheimer’s disease and distinguish AD from other types of dementia“A usually progressive condition (such as Alzheimer's disease) marked by the development of multiple cognitive deficits such as memory impairment, aphasia, and the inability to plan and initiate complex behavior.”10. An additional cause of Alzheimer’s disease is abnormal tau proteinA protein that helps stabilize the structure of a neuron and facilitate the transportation of nutrients and other essential molecules. In unhealthy amounts, tau proteins cling to one another instead, creating protein clumps known as neurofibrillary tangles. These neurofibrillary tangles, made up of tau proteins, disrupt neural functions and are a risk factor for AD.22, 23 production. This protein is a key component of microtubules, which transport nutrients between nerve cells. Thus, abnormal tau protein production threatens microtubule structures and increases the risk of AD.33
While Alzheimer’s is the most common type of dementia“A usually progressive condition (such as Alzheimer's disease) marked by the development of multiple cognitive deficits such as memory impairment, aphasia, and the inability to plan and initiate complex behavior.”10,34 dementia is an umbrella term for memory loss and other impairments to an individual’s cognitive function. Dementia leads to decreased ability to perform activities of daily living.35 The term refers to several types, such as Lewy body dementia, frontotemporal dementia, mixed dementia, Parkinson’s disease dementia, Alzheimer’s diseaseA degenerative brain disease and the most common form of dementia.1, and others.36, 37
Q: How is Alzheimer’s diagnosed?
A: The stages of Alzheimer’s diseaseA degenerative brain disease and the most common form of dementia.1, from the mildest to the most severe stages, are termed as follows: cognitively normal, significant memory concern, early mild cognitive impairment, mild cognitive impairment (MCI), mild dementia“A usually progressive condition (such as Alzheimer's disease) marked by the development of multiple cognitive deficits such as memory impairment, aphasia, and the inability to plan and initiate complex behavior.”10, late mild cognitive impairment, and full Alzheimer’s disease.38 Alzheimer’s disease is often diagnosed during the mild dementia stage, in which it becomes evident to family and doctors that the patient has “significant trouble with memory and thinking that impacts daily functioning.”39 Computed tomography (CT) scans can be used to diagnose Alzheimer's disease definitively, or the disease“A condition that impairs normal functioning and is typically manifested by distinguishing signs and symptoms.”11 can be suspected based on medical history, characteristic changes in thinking, physical examinations, and laboratory tests.40
Identifying the disease“A condition that impairs normal functioning and is typically manifested by distinguishing signs and symptoms.”11 is arduous, particularly since Alzheimer’s results in several complications that may hide the disease. The plaques indicative of Alzheimer’s diseaseA degenerative brain disease and the most common form of dementia.1 are not fatal in and of themselves. Still, the nerve connections that AD destroys in the brain make ordinary tasks difficult and unfamiliar. Complications are common among patients with Alzheimer’s, as neurodegeneration leads to physical effects. Many persons whose underlying cause of death is Alzheimer's die from a complication due to Alzheimer's.41 In 2021 alone, over 120,000 deaths were attributed to AD.42 Complications may include vascular changes, aspiration pneumonia, bedsores, sepsis infections from undiagnosed urinary tract infections, infections in general, injuries from falls, malnutrition, and dehydration.
Q: What are the risk factors for developing Alzheimer’s disease?
A: Many risk factors“A factor, such as a habit or an environmental condition, that predisposes an individual to develop a particular disease.”21 contribute to the possibility of an individual developing AD, some of which an individual can somewhat control (modifiable factors) and some which an individual cannot control (nonmodifiable factors). Nonmodifiable risk factors, which increase an individual’s risk of developing Alzheimer’s, include age, sex, family history, race, and genetics. The research discusses extensively how nonmodifiable risk factors correlate with Alzheimer’s.43 However, several studies suggest a strong correlation between increased risk of AD and the presence of somewhat-modifiable factors, such as chronic high blood pressure,44, 45, 46 various heart diseases,47, 48 high cholesterol,49, 50 and diabetes.51, 52, 53 For instance, chronic high blood pressure promotes plaque buildup, known as Atherosclerosis“The build-up of fats, cholesterol and other substances in and on your artery walls (plaque), which can restrict blood flow.”5, which can kill cortical tissue and ultimately lead to cognitive impairment.54 Simultaneously, regular exercise, a low-salt diet, and other health-promoting treatments can treat chronic high blood pressure.55 This brief will further discuss modifiable risk factors for AD in the Contributing Factors section.
Q: Who is most likely to be affected by Alzheimer’s disease?”
A: AD is much more likely to affect those who are older; popular statistics indicate that once an individual reaches the age of 65, their risk of developing Alzheimer’s doubles every five years.56 Additionally, nearly two-thirds of those diagnosed with AD in the United States are women.57 Recent studies indicate women may be more likely to develop AD because women tend to live longer than men, and the hormone changes that occur in many women’s bodies due to aging may make females more susceptible to developing the amyloid plaques characteristic of AD.58 For women or men who carry the apolipoprotein-e4 (APOE-e4) alleleOne variation of the Apolipoprotein-e gene, which involves the metabolism and repairing of cell membranes in the central and peripheral nervous systems. This allele most likely contributes to plaque buildup and neurofibrillary tangles, both risk factors for developing Alzheimer’s Disease.4, the risk of developing AD (and developing AD earlier) is higher than for individuals who do not carry the allele.59, 60

Race has also been a noted nonmodifiable risk factor in the development of AD; studies indicate that in the United States, African American and Latinx individuals are more likely to develop AD than individuals of European or American heritage.61, 62 There are many theories for why this is the case, including the hypothesis that African American and Hispanic individuals are more likely to carry the APOE-e4 alleleOne variation of the Apolipoprotein-e gene, which involves the metabolism and repairing of cell membranes in the central and peripheral nervous systems. This allele most likely contributes to plaque buildup and neurofibrillary tangles, both risk factors for developing Alzheimer’s Disease.4 that leaves them more susceptible to developing AD.63, 64 However, we note that there are significant criticisms of the designs used to determine statistics on AD, the most notable being that medical research in the past has not appropriately accommodated minorities and, as a result, may lead to misdiagnosis and mistreatment in medicine.65
Given the complex nature of mental health issues, it is unclear how much mental health issues such as depression independently correlate with increased risk of AD.66, 67 However, one study notes that patients with severe depression were 2.7 times more likely to be diagnosed with dementia“A usually progressive condition (such as Alzheimer's disease) marked by the development of multiple cognitive deficits such as memory impairment, aphasia, and the inability to plan and initiate complex behavior.”10 in the next 3 years.68
Q: Has Alzheimer’s become more prevalent in recent years?
A: Since its discovery in 1906, Alzheimer’s diseaseA degenerative brain disease and the most common form of dementia.1 has become increasingly prevalent among adults in the United States. Today, the CDC estimates that 5.4 million people in the US have Alzheimer’s disease.69 Meanwhile, a report from the Alzheimer’s Association estimates that 6.5 million adults over the age of 65 have AD in the United States and reports that each year, 100,000 people develop AD.70 Some studies estimate that by 2050, 14 million people will have AD.71, 72, 73 Because research methods to identify and diagnose AD is improving, Alzheimer’s disease most likely will continually become more prevalent in the future.

Alzheimer’s diseaseA degenerative brain disease and the most common form of dementia.1 is currently the sixth-leading cause of death in the United States and is the fifth-leading cause of death for those ages 65 and older,74 killing more than breast cancer and prostate cancer combined each year.75 By 2040, approximately one in five Americans will be age 65 or older, rising from one in eight in 2000.76 Current projections estimate that in 2050, 1.6 million people in the US could die due to AD, a number that is nearly triple the number of recorded AD deaths in 2010.77, 78
Interestingly, research continues to debate whether the actual risk of developing AD will increase, decrease, or remain constant in the US. Several studies indicate that in the last 25 years, the actual risk of developing Alzheimer’s diseaseA degenerative brain disease and the most common form of dementia.1 has either remained stable or declined in the United States and in other Western countries.79 Researchers have attributed the decline to several factors, such as improvements in education and more excellent controls over cardiovascular risk factors“A factor, such as a habit or an environmental condition, that predisposes an individual to develop a particular disease.”21.80 Other studies argue that the risk has held constant in the last 20 years and will continue to do so.81 Overall, the risk of AD may be declining or holding constant, AD’s prevalence in the US continues to rise as more adults age into their senior years.
Q: Is there a cure or treatment for Alzheimer’s?
A: There is currently no sure way to prevent or cure this disease“A condition that impairs normal functioning and is typically manifested by distinguishing signs and symptoms.”11.82 Current management of the disease includes five FDA-approved drugs, many of which temporarily improve cognitive symptoms for patients.83 There are currently no drugs that are FDA approved to treat behavioral and psychiatric symptoms that often develop in patients with Alzheimer’s diseaseA degenerative brain disease and the most common form of dementia.1.84 Despite the spending of billions of dollars on research, no cure or permanent means for slowing down the disease exists.85 However, the identification of varying degrees of Alzheimer’s disease has encouraged more significant attention to preventative measures.
Q: How does this issue look today?
A: There is still room for improvement in the care and resources provided for Alzheimer’s patients and their caregivers, as well as the efficiency with which healthcare professionals detect and diagnose the disease“A condition that impairs normal functioning and is typically manifested by distinguishing signs and symptoms.”11. Currently, outside of research settings, many individuals who should be diagnosed with Alzheimer’s diseaseA degenerative brain disease and the most common form of dementia.1 are not getting the diagnosis they need—being underdiagnosed, misdiagnosed, or undiagnosed because physicians avoid prematurely diagnosing Alzheimer’s disease without a full diagnostic workup.86 In 2016, there was “one geriatrician for every 1,924 Americans age 65 or older in need of care.”87 Far from the recommended ratio of 1 geriatrician per 3 or 4 patients, this 2016 figure indicates that the United States health system does not have enough trained geriatric healthcare professionals to meet the need of the increasing prevalence of Alzheimer’s disease in America.88, 89

Contributing Factors
Lifestyle Choices
Lifestyle choices, such as physical activity and stress management, contribute to the prevalence of AD because these behaviors impact an individual’s risk of developing AD. Recent research demonstrates that key factors contributing to the development of chronic illnessesMedical conditions that last one year or more and require ongoing medical attention. Examples of chronic illnesses include arthritis, asthma, diabetes, and heart disease.8 such as Alzheimer’s include “high blood pressure, tobacco smoking and second-hand smoke exposure, high body-mass index (BMI), physical inactivity, alcohol use, and diets low in fruits and vegetables and high in sodium and saturated fats.”90 While not the only risk factor for AD, lifestyle choices makeup approximately 35% of dementia“A usually progressive condition (such as Alzheimer's disease) marked by the development of multiple cognitive deficits such as memory impairment, aphasia, and the inability to plan and initiate complex behavior.”10 cases and thus are important modifiable risk factors“A factor, such as a habit or an environmental condition, that predisposes an individual to develop a particular disease.”21.91 Furthermore, addressing these lifestyle choices can seriously reduce individual and societal AD risk, given the prevalence of these choices in the US. One report estimates that reducing these modifiable behaviors even by 10% to 25% can prevent as many as 3 million cases of AD worldwide.92 Thus, these modifiable risk factors impact the prevalence of AD in the US.

Physical Inactivity
Physical inactivity has long-term impacts on cognitive activity and the risk for AD. In the US, over 60% of adults do not engage in the recommended amount of daily physical activity, which is either 30 minutes of moderate activity (such as brisk walking) or 15–20 minutes of strenuous activity (such as jogging or running).93 Research demonstrates that physical activity, even regular walking, is associated with greater gray matterTissue that makes up the outermost layer of the human brain. This brain tissue exists along the brain, brain stem, and spinal cord. Gray matter is dense in unmyelinated axons (creating its pinkish gray tone), whereas white brain matter is composed of myelinated axons. Gray matter contains networks of neurons that are responsible for essential motor functions.13, 14 in several brain areas, improving brain function. Physical activity also increases the size of the hippocampus–a region of the brain responsible for memory formation.94 One study examined AD patients who did not exercise regularly and AD patients who did regular exercise. The researchers found that AD patients who did not regularly exercise had a 1.5% decline in the size of their hippocampus, while AD patients who did regular exercise had a 2% increase in the size of their hippocampus.95 While not a perfect solution, the increased size of certain brain areas, including the hippocampus, leads to improved cognitive function. Other studies support the correlation between regular physical activity and improved memory and cognitive function.96 One study noted that 1 year of regular, moderately intense exercise (40 minutes a day, 3 days a week) increased spatial memory in healthy older adults and led to reductions in memory impairment.97, 98 For US adults, regular physical exercise can significantly reduce the risk of AD and improve the quality of life for individuals with AD. One study from 2020 estimates that individuals who exercise regularly reduce their risk of developing AD by approximately 45%.99 Therefore, physical activity substantially impacts one’s risk for and experience with Alzheimer’s.
Poor Stress Management
Prolonged stress poses an additional risk to the development and severity of AD in adults.100 In recent surveys, only 28% of adults in the US reported managing their stress well through mediums like listening to music, exercising, meditating, and spending time with loved ones.101 In a 2019 poll, 55% of adults in the US said they experienced stress during “a lot of the day” compared to 35% of adults globally.102 Research demonstrates that chronic strain drives the progression of several diseases and worsens symptoms because of increased cortisolThe body’s primary stress hormone. Cortisol increases glucose levels and, when at chronically high levels, can alter the body’s immune system response and increase the risk of various diseases.9 levels.103, 104, 105, 106 This behavior occurs for cardiovascular diseases, cancers, neurodegenerative diseases such as AD, and other conditions. These various diseases, alongside exacerbating stress and cortisolThe body’s primary stress hormone. Cortisol increases glucose levels and, when at chronically high levels, can alter the body’s immune system response and increase the risk of various diseases.9, then disrupt healthy stress circuits, increasing stress and leading to further complications such as depression, anxiety, and aggressive behavior.107 As for AD, studies with mice and rats reveal that exposure to stressors increased the production of Aβ, leading to greater amyloid plaque buildup and neurodegeneration.108, 109 These elevations persisted for up to 12 months after researchers exposed the animals to stress.110, 111 In a similar pattern, tau proteinA protein that helps stabilize the structure of a neuron and facilitate the transportation of nutrients and other essential molecules. In unhealthy amounts, tau proteins cling to one another instead, creating protein clumps known as neurofibrillary tangles. These neurofibrillary tangles, made up of tau proteins, disrupt neural functions and are a risk factor for AD.22, 23 tangles associated with AD risk were also exacerbated by prolonged stress, leading to increased production of Aβ and eventual neurodegeneration. Thus, prolonged strain alters the body’s normal processes and increases the risk of several diseases, including AD.
Further research demonstrates how stress rapidly progresses AD and other dementias by elevating levels of cortisolThe body’s primary stress hormone. Cortisol increases glucose levels and, when at chronically high levels, can alter the body’s immune system response and increase the risk of various diseases.9.112 Although research has yet to determine if effective stress management decelerates the progression of AD, several studies note that it is still beneficial to individuals with AD.113 For instance, stress management may lower stress hormones and amyloid production, thus slowing cognitive decline.114, 115, 116 Considering that the prevalence of anxiety is reportedly higher in elderly adults than in younger age groups (approximately 15% of all older adults globally),117 poor stress management may increase the severity and prevalence of AD for adults in the US.118
Social Interaction
Alongside lifestyle choices, one’s quality of personal relationships impacts one’s overall cognitive health and risk of AD. Generally, supportive relationships and a rich social network—networks in which an individual maintains long-term, positive, and supportive relationships with others—are key factors to improved cognitive function and lower cognitive decline in older adults.119, 120, 121 One study found that healthy social networks disrupt the relationship between cognitive function and dementia“A usually progressive condition (such as Alzheimer's disease) marked by the development of multiple cognitive deficits such as memory impairment, aphasia, and the inability to plan and initiate complex behavior.”10, where cognitive function remained higher for participants who reported strong social networks.122 Unfortunately, research on the exact relationship between social networks and biological processes surrounding dementia risk is inconclusive. However, one study reported a statistically significant relationship between social network quality and the density of neurofibrillary tanglesAbnormal accumulations of tau proteins inside neurons, which damages neural networks and prevents the brain from communicating properly. The abnormal accumulations most often reside in brain areas involved in memory.16, where the decreased quality of relationships correlated with increased tangle density and increased AD risk.123 Therefore, strong social networks are a factor in the prevalence of AD.

Photo by A Koolshooter
Extensive research supports a negative correlation between the risk of AD and the extent of one’s contact with loved ones.124, 125, 126 Similarly, feelings of loneliness are associated with an increased risk of dementia“A usually progressive condition (such as Alzheimer's disease) marked by the development of multiple cognitive deficits such as memory impairment, aphasia, and the inability to plan and initiate complex behavior.”10, including AD.127, 128 In one study, elderly participants who reported satisfaction in their relationships had a 23% reduced risk of AD, and participants who reported “[emotionally] receiving more than they gave” had a 53% reduced risk of AD.129 These findings have serious implications for reducing the prevalence of AD in the United States. However, we note that measures of healthy social networks are inconsistent in existing research. For instance, studies may utilize marital status, frequency of contact with loved ones, perceptions of relationship quality, number of loved ones, overall satisfaction, or a combination of these measures.130 Therefore, while the quality of relationships influences dementia risk, these individual measures of healthy social networks may influence overall risk at varying levels.
Environmental Factors
Environmental factors such as air pollution contribute to the prevalence of AD because such external factors influence one’s internal processes, including one’s nervous system. More specifically, exposure to toxic air pollutants leads to AD by accelerating Aβ accumulation 131 and prompting other AD-specific processes.132, 133, 134 Air pollution includes various particles, such as particulate matter (PM), gases (e.g., ground-level ozone, carbon monoxide), organic compounds, metals, etc.135, 136 These particles can have effects on an individual at all stages of human development, culminating in various diseases.137 For example, PM is made of organic and inorganic materials and can originate from road and agricultural dust, refineries, power plants, mobile sources, construction, and other common sources.138 PM is associated with respiratory damage and brain inflammation, leading to neuron damage and an increased risk of AD (along with other conditions, such as cardiovascular diseases).139, 140, 141 Overall, an estimated 135 million Americans live in regions with unhealthy levels of ozone and air pollution.142 Given that an estimated 67 million tons of pollution were emitted in the US in 2021, air pollution continues to be relevant to the issue of AD.143
Exposure to toxic air pollutants leads to AD through several processes–namely, by accelerating Aβ accumulation,144 prompting abnormal production of the tau proteinA protein that helps stabilize the structure of a neuron and facilitate the transportation of nutrients and other essential molecules. In unhealthy amounts, tau proteins cling to one another instead, creating protein clumps known as neurofibrillary tangles. These neurofibrillary tangles, made up of tau proteins, disrupt neural functions and are a risk factor for AD.22, 23, and inducing neuroinflammationAn inflammatory response in the brain or spinal cord. While low levels of neuroinflammation can benefit the body’s immune system and brain function, severe neuroinflammation can lead to tissue damage, stress, and cell death.17, 18 and oxidative stress.145, 146, 147 Each of these processes is a key indicator of AD risk, as discussed earlier. One study suggested that exposure to air pollutants may lead to premature aging and disease“A condition that impairs normal functioning and is typically manifested by distinguishing signs and symptoms.”11 progression.148 For individuals in urban areas, these effects are particularly prevalent.149, 150 For instance, one study found that participants in urban areas, where air pollutants are more prevalent, had more abnormalities in expressing the APOE-e4 alleleOne variation of the Apolipoprotein-e gene, which involves the metabolism and repairing of cell membranes in the central and peripheral nervous systems. This allele most likely contributes to plaque buildup and neurofibrillary tangles, both risk factors for developing Alzheimer’s Disease.4 and producing the tau proteinA protein that helps stabilize the structure of a neuron and facilitate the transportation of nutrients and other essential molecules. In unhealthy amounts, tau proteins cling to one another instead, creating protein clumps known as neurofibrillary tangles. These neurofibrillary tangles, made up of tau proteins, disrupt neural functions and are a risk factor for AD.22, 23. Of these individuals, 51% also had Aβ plaque buildup.151, 152 Therefore, the prevalence of air pollution in the US correlates with the prevalence of AD in the US, given pollutants’ effects on an individual’s internal processes.
Consequences
High Mortality and Morbidity Rate
The prevalence of Alzheimer’s in the US leads to an increase in morbidityThe condition of ill health or disease.15 and mortality rates because AD and other dementias directly lead to life-threatening medical complications. This process is known as the Alzheimer’s diseaseA degenerative brain disease and the most common form of dementia.1 continuum, where the degenerative changes made to the brain as a result of Alzheimer’s disease cause problems with memory and eventually lead to physical disability.153, 154 The AD continuum begins with the phase of preclinical Alzheimer’s, which manifests no symptoms, and continues until the individual has severe Alzheimer’s disease, where the patient needs around-the-clock care to complete tasks involved in daily living—a process spanning an average of 4–8 years.155, 156 An individual with Alzheimer’s may experience complications such as immobility, malnutrition, and swallowing disorders“An abnormal physical or mental condition.”12. Alzheimer’s may also compromise an individual’s immune system response, leading to conditions like pneumonia, which is commonly identified as the immediate cause of death among older Americans with dementia“A usually progressive condition (such as Alzheimer's disease) marked by the development of multiple cognitive deficits such as memory impairment, aphasia, and the inability to plan and initiate complex behavior.”10.157
In recent years, the prevalence of Alzheimer’s in the US has led to increased deaths due to AD. In the United States in 2000, there was a noted 17.6 deaths due to AD per 1,000 deaths; in 2018, there were 37.3 AD deaths per 1,000 deaths.158 Instead of concluding that this trend is evidence of AD becoming more deadly, it would be more appropriate to associate this trend with our increased understanding of AD and its effects on the human body. Increased medical understanding has likely led to an increase in pronouncing AD as the cause of death on death certificates.159

Photo by Muskan Anand
Negative Economic Impact
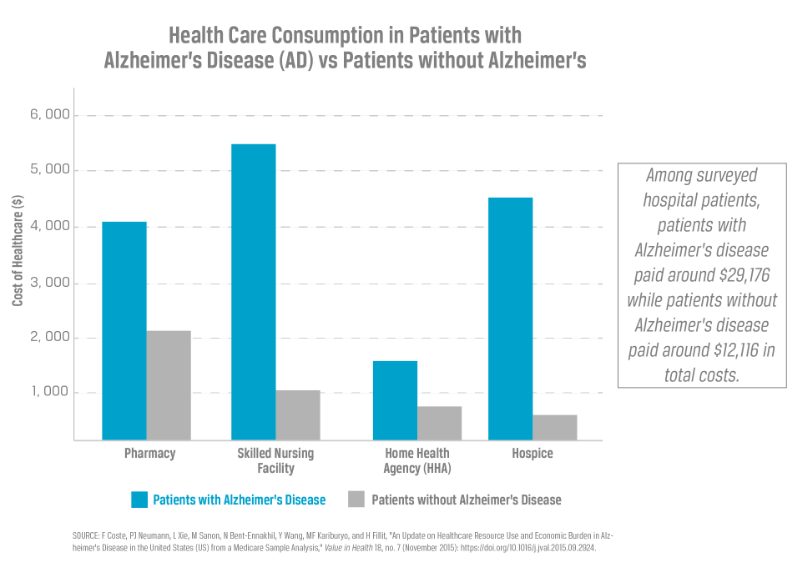
The prevalence of Alzheimer’s also leads to negative economic impacts, as the public typically funds long-term care and healthcare payments in the form of Medicare, Medicaid, and Social Security. In a Medicare sample analysis conducted in 2015, patients with Alzheimer’s had significantly more costs per patient-per-year health care consumption in inpatient facilities than patients without Alzheimer’s. One study found that older patients with AD incurred higher annual healthcare costs in several categories: hospice care, inpatient services, pharmacy, emergency, ambulatory care, and others. For instance, older patients with AD incurred total annual costs of approximately $29,176, whereas older patients without AD incurred an average of $12,116.160
Alzheimer’s patients also incurred significantly higher inpatient, pharmacy, and total costs.161 One report estimated that the cost of caring for individuals with Alzheimer’s in 2020 was $305 billion. Of this amount, $206 billion, or 67%, is expected to be covered by Medicare and Medicaid. Another report estimates that by 2050, expenses due to Alzheimer’s (such as expenses for trained medical care and medication) will increase Medicare and Medicaid costs by over 330%.162 This increase indicates that without a successful cure, the annual out-of-pocket payments for Alzheimer’s and dementia“A usually progressive condition (such as Alzheimer's disease) marked by the development of multiple cognitive deficits such as memory impairment, aphasia, and the inability to plan and initiate complex behavior.”10 care in the US are projected to reach $1.1 trillion in total by 2050.163 These statistics point, not only to a rise in the disease itself, but also to a rise in the cost of care and the need for trained medical staff to meet the growing demand.
Caregiver Burden
Caregivers to those with Alzheimer’s are also negatively affected when the disease progresses because they bear much of the economic and emotional burden of care. Economic burden relates to the financial costs and hardships of caring for an individual with ASD.164, 165 In the United States, 83% of older adults (with and without AD) are looked after by a friend or family member rather than a paid caregiver.166 In 2015, this percentage equated to approximately 15 million family members and other unpaid caregivers, who provided an estimated 18.1 billion hours of unpaid care to individuals with Alzheimer’s and other dementias.167 These hours equate to an economic burden valued at over $244 billion.168 These hours may be spent providing direct and indirect care, such as cooking for the patient, administering medications, and assisting the patient around the house.169 Surveyed family caregivers reported opting to provide care for various reasons, including keeping the loved one with dementia“A usually progressive condition (such as Alzheimer's disease) marked by the development of multiple cognitive deficits such as memory impairment, aphasia, and the inability to plan and initiate complex behavior.”10 at home and close, particularly when the loved one was a spouse or partner.170
Caregiving can be a rewarding experience, as it allows the caregiver to maintain close intimacy with a family member or friend near the end of the family member’s life.171 However, many caregivers describe their experience as distressful, particularly when the patient resists caregiver assistance. This resistivenessAny opposition to care, typically during an encounter between a caregiver and care recipient.20 is a well-known behavioral and psychological symptom of Alzheimer’s diseaseA degenerative brain disease and the most common form of dementia.1, in addition to agitation and aggression.172 In 2015, nearly 60% of Alzheimer's and dementia“A usually progressive condition (such as Alzheimer's disease) marked by the development of multiple cognitive deficits such as memory impairment, aphasia, and the inability to plan and initiate complex behavior.”10 caregivers rated the emotional stress of caregiving as high or very high, 40% reported symptoms of depression, and 36% of caregivers die before the person they are caring for.173 When compared to caregivers of patients with schizophrenia (20%), caregivers of patients with dementia report a higher prevalence of depression (30% to 40%).174 Caregivers for individuals with dementia lose an estimated 2.4–3.5 hours of sleep each week due to prolonged stress and concern for their loved ones with dementia.175
Due to the physical and emotional toll of caregiving, AD and dementia caregivers in the United States have approximately $9.7 billion in additional health care costs, which include medication, exams, Medicare expenses, and others. Forty-one percent of caregivers have a household income of $50,000 or less, meaning total annual costs of approximately $29,000 makes up a significant amount of yearly expenses.176

Practices
Wellness Programs
Beyond just physical activity, wellness is defined by the Global Wellness Institute as “the active pursuit of activities, choices, and lifestyles that lead to a state of holistic health.” Overall wellness is crucially impacted by the cultural, physical, and social environments in which we live.177 In the past few decades, researchers have examined the relationship between positive wellness choices and Alzheimer’s diseaseA degenerative brain disease and the most common form of dementia.1 risk. For instance, a 2006 study enrolled participants in wellness activities to promote self-control, physical exercise, mental stimulation, and social interaction.178 Compared to a control group, participants involved in the art programs showed better health, higher morale, fewer depressive symptoms, and greater protection against dementia“A usually progressive condition (such as Alzheimer's disease) marked by the development of multiple cognitive deficits such as memory impairment, aphasia, and the inability to plan and initiate complex behavior.”10 and cognitive decline.179 Just a year into the study, groups involved showed stabilization and improvement in cognitive decline, indicating a decreased severity of AD symptoms and a potentially decreased risk of Alzheimer’s disease.
In 2018, the Alzheimer’s Association announced its latest clinical study, The US Study to Protect Brain Health Through Lifestyle Intervention to Reduce Risk (US POINTER). This 2-year nationwide clinical study examines exactly how lifestyle choices protect cognitive function and memory in older adults.180 Modeled after a 2014 clinical trial in Finland, POINTER tests a combination of wellness practices, including a healthy diet, physical activity, cognitive exercises, and social activities, and their effect on AD risk.181 The study, which officially began in 2019, enrolled 2,000 older American adults (60–75 years old) who may be at risk for dementia“A usually progressive condition (such as Alzheimer's disease) marked by the development of multiple cognitive deficits such as memory impairment, aphasia, and the inability to plan and initiate complex behavior.”10.182 Participants are provided resources and tools to complete the 2-year lifestyle program and are required to receive regular checkups and evaluations on their physical and mental health. These evaluations include measures for episodic memory, executive function, processing speed, the severity of dementia risk, functional ability, and other measures.183 While this study will not be completed until 2024 due to the COVID-19 pandemic, US POINTER represents the first nationwide study on the relationship between Alzheimer’s diseaseA degenerative brain disease and the most common form of dementia.1, brain health, and wellness choices.184, 185 Given the study’s emphasis on including sufficient numbers of Black, Hispanic, Asian, and Native Americans as study participants, these results will provide a unique perspective on the prevalence of AD in the US.186, 187
Preferred Citation: George, Margaret and Erica Bassett. “Prevalence of Alzheimer’s Disease in Adults in the United States.” Ballard Brief. September 2022. www.ballardbrief.byu.edu.
Viewpoints published by Ballard Brief are not necessarily endorsed by BYU or The Church of Jesus Christ of Latter-day Saints