
Prevalence of Non-Communicable Disease among Adults in Tonga


By Autumn Vaitohi
Published Fall 2022
Special thanks to Seth Ririe for editing and research contributions.
Viewpoints published by Ballard Brief are not necessarily endorsed by BYU or The Church of Jesus Christ of Latter-day Saints.
Summary+
Non-communicable diseases, or NCDs, are a primary health issue among people in the South Pacific country of Tonga. This issue is driven by various factors, the most notable being poor consumption behaviors, sedentary living, and genetics specific to this demographic. As a result of NCDs in Tonga, the population is experiencing high morbidity and mortality rates and a decreased stability of the healthcare system, government, and economy. Therefore, implementing interventions that are multifaceted and able to address all aspects, social, legislative, physiological, environmental, and so on, of the issue is key to finding success in overcoming this health issue.
Key Takeaways
99.9% of Tongans engage in behaviors that put them at risk for developing NCDs.
Tonga is facing NCD mortality at a rate 13% higher than the global average while in an earlier stage of economic development than much of the world. Because of this, they have limited resources and less time to adequately respond to the alarming growth of NCDs. 118
Research supports that Tongans may be more likely to develop NCDs due to their genetic makeup.
Those in urban areas are at an increased risk for NCDs because they have increased access to imported goods.
The best practices to combat this problem include improving legislation surrounding NCD-related laws.
Key Terms+
Body Mass Index (BMI)—The most common tool for determining obesity. Based on a person's weight and height, they are given a number; if a person’s BMI number reaches 30 or above, they are considered obese.1
Diabetes Mellitus (DM)—Includes both type 1 and type 2 Diabetes Mellitus. Type 1 DM is different from type 2 in that it is an autoimmune disorder developed solely due to a person's genetics rather than lifestyle choices.
Free Sugar—All sugars added to foods or drinks by the manufacturer, cook, or consumer, as well as sugars naturally present in honey, syrups, fruit juices, and fruit juice concentrates.2
Health promotion—The process of enabling people to increase control over, and to improve, their health—moving beyond individual behavior and towards a wide range of social and environmental interventions.3
Homeostasis—The tendency towards a relatively stable equilibrium between interdependent elements, especially maintained by physiological processes.4
Ischemic Heart Disease—A disease that develops due to a buildup of plaque on the walls of the heart arteries, which are responsible for supplying blood to the heart muscle. An excess of cholesterol in the blood commonly forms this plaque. This disease is also known as coronary heart disease (CHD) or coronary artery disease.5
Morbidity—General disease or suffering that occurs because of a medical condition.
Mortality—Refers to death or the state of being subject to death.
Mutton flaps—A cut of meat from a lamb's breast known for its relatively low cost and high-fat content.6
Non-communicable disease (NCD)—A health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7
Obesity—A disease primarily characterized by an excessive amount of body fat. It is most frequently determined by a measurement of weight that is considered too high compared to a person's height.
Triglycerides—The most common form of fat found in the body. They can come directly from high-fat foods, or are formed from excess consumption of calories.8
Type II Diabetes Mellitus (T2DM)—A chronic condition characterized by excess sugar in the bloodstream. Decreased pancreatic and cellular functions decrease the body’s ability to utilize glucose as a primary energy source. Left untreated, it can lead to severe malfunctions of the primary body systems.9
Context
Q: What are non-communicable diseases (NCDs) and which are of the greatest concern in Tonga?
A: A non-communicable diseaseA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7 (NCD) is a health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors such as high blood pressure, high blood glucose levels, and high cholesterol.10 Rather than measuring NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7 by their overall prevalence, NCDs are generally measured by the prevalence of risk factors and NCD-related mortality rates. Risk for NCDs is determined by factors such as daily smoking, alcohol consumption, being overweight, having raised blood pressure, having consumed low nutritional foods, and having engaged in low activity levels.11 Due to limited access to healthcare, many of these NCDs are associated with high levels of morbidityGeneral disease or suffering that occurs because of a medical condition. and mortalityRefers to death or the state of being subject to death..12

There are a variety of NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7 that are currently threatening the Kingdom of Tonga. Those of greatest concern include cardiovascular disease (CVD), diabetesIncludes both type 1 and type 2 Diabetes Mellitus. Type 1 DM is different from type 2 in that it is an autoimmune disorder developed solely due to a person's genetics rather than lifestyle choices., obesityA disease primarily characterized by an excessive amount of body fat. It is most frequently determined by a measurement of weight that is considered too high compared to a person's height., respiratory disease, and cancer. The 2017 STEPS report, conducted in collaboration with the World Health Organization, indicated that 99.9% of the population in Tonga was at either moderate or high risk of NCDs.13 Recent studies show that approximately 74% of all deaths in Tonga can be attributed primarily to NCDs.14
Researchers have found that the development of one NCD can increase the risk of developing other NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7. One especially important NCD which leads to others is obesityA disease primarily characterized by an excessive amount of body fat. It is most frequently determined by a measurement of weight that is considered too high compared to a person's height.. Throughout this paper, the term ‘obesity’ refers to an NCD while the term ‘overweight’ refers to a risk factor of NCDs. The two are differentiated by BMIThe most common tool for determining obesity. Based on a person's weight and height, they are given a number; if a person’s BMI number reaches 30 or above, they are considered obese.1: individuals with a BMI greater than or equal to 25 are classified as overweight, while those with a BMI greater than or equal to 30 are classified as obese.15
Q: Who is most at risk of developing NCDs in Tonga?
A: The entire population of Tonga is at risk for developing NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7. A survey conducted among Tongans aged 18–69 found that 99.9% of the population was at risk for NCDs and that the number of risk factors increased with age. The percentage of individuals with 1–2 risk factors is higher among Tongans aged 18–29 (43.1%) than aged 45–69 (25.0%). However, the percentage of Tongans with 3–5 risk factors was higher among the older group (aged 45–69) at 74.8% than those aged 18–29 (56.7%).16 Due to the growing risk of NCDs and their subsequent consequences as the population ages, this paper focuses primarily on NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7 among the adult population in Tonga.

There is also data that suggests that individuals living in urban areas are at higher risk of exposure to certain NCD risk factors, such as consuming higher amounts of low-nutritional foods. Development and urbanization, including the shift away from traditional diets, are associated with increased rates of obesityA disease primarily characterized by an excessive amount of body fat. It is most frequently determined by a measurement of weight that is considered too high compared to a person's height., diabetesIncludes both type 1 and type 2 Diabetes Mellitus. Type 1 DM is different from type 2 in that it is an autoimmune disorder developed solely due to a person's genetics rather than lifestyle choices., and cardiovascular disease.17 This shift is likely due to the increased availability of imported goods to those living in more developed areas.
Q: How has the prevalence of NCDs in Tonga changed over the most recent decades?
A: Due to a lack of data collection over the most recent decades, only the current prevalence of select NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7 is available. Data collecting on the prevalence of NCDs at specific points in time is rare because the diseases are most commonly measured by death rates and prevalence of risk factors rather than the prevalence of the actual disease. This collection is likely due to benchmarks such as the sustainable development goal set forth by the WHO, which aims to reduce the prevalence of NCDs by one-third by 2030 and reviews NCD mortalityRefers to death or the state of being subject to death. rates to measure this goal.18 Using mortality rates to measure the prevalence of NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7 is a straightforward process that allows for greater accuracy than the process of diagnosing and documenting NCDs among the entire adult Tongan population. Among the information available for Tonga is data collected from 1973 to 2012 that shows the rate of type-two diabetes mellitus (T2DMA chronic condition characterized by excess sugar in the bloodstream. Decreased pancreatic and cellular functions decrease the body’s ability to utilize glucose as a primary energy source. Left untreated, it can lead to severe malfunctions of the primary body systems.9) growing from 5.2% to 19% and obesityA disease primarily characterized by an excessive amount of body fat. It is most frequently determined by a measurement of weight that is considered too high compared to a person's height. prevalence growing from 56% to 70.2% among adults aged 25–64.19 While obesity is classified as an NCD, its presence commonly contributes to the development of other NCDs, meaning that those diagnosed with obesity are more likely to have other NCDs as well. Being overweight is a primary risk factor for the development of NCDs, including obesity. Because the prevalence of overweight and obesityA disease primarily characterized by an excessive amount of body fat. It is most frequently determined by a measurement of weight that is considered too high compared to a person's height. has increased over the past several decades, it is reasonable to conclude that the overall prevalence of NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7 has grown significantly during that same time since obesity is directly related to the occurrence of diabetesIncludes both type 1 and type 2 Diabetes Mellitus. Type 1 DM is different from type 2 in that it is an autoimmune disorder developed solely due to a person's genetics rather than lifestyle choices., cardiovascular disease, and cancer.20
In 2005, Tonga joined the World Trade Organization, ultimately reducing the cost of tariffs and reducing their reliance on the domestic market. This shift in the availability of international food has caused citizens to deviate from eating domestic foods in preference for corned beef, mutton flapsA cut of meat from a lamb's breast known for its relatively low cost and high-fat content.6, refined carbohydrates, and other foods that are abundant in unhealthy nutrients.21 These imported goods stand in stark contrast to local goods that were previously consumed, such as fish or indigenous chicken—lean proteins that are now 15–50% more expensive than the imported, high-fat proteins.22 Data for Tonga shows that higher rates of obesityA disease primarily characterized by an excessive amount of body fat. It is most frequently determined by a measurement of weight that is considered too high compared to a person's height., diabetesIncludes both type 1 and type 2 Diabetes Mellitus. Type 1 DM is different from type 2 in that it is an autoimmune disorder developed solely due to a person's genetics rather than lifestyle choices., and cardiovascular disease are correlated with the increased availability and consumption of imported goods.23 Furthermore, there has been a recorded increase in energy intake from imported foods from 31% to 50% from 1980 to 2006 in Tonga.24 While this data may seem outdated, it is important to note that 99.9% of Tongans are cited as being at moderate to high risk for developing NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7 since the initial STEPS report in 2004 up until the most recent report in 2017. This data remains relevant because of the correlation that exists between NCDs and the availability of imported goods. It is clear that the growing prevalence of imported foods is not only making poor diet choices more accessible and affordable to the general population but is directly associated with an increased rate of NCDs in Tonga over the past several decades.25
Q: How does the prevalence of NCDs in Tonga compare with that of the rest of the world?
A: In the 2020 Non-communicable Diseases Progress Monitor report by the World Health Organization, it was indicated that NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7 are responsible for just over 70% of deaths worldwide. Within this statistic, it was also reported that 83% of deaths in Tonga occurred from a NCD. Sitting 13% above the global average, Tonga also has a relatively high probability of premature mortalityRefers to death or the state of being subject to death. from NCDs, as 23% of the population is expected to suffer a premature death due to NCDs—almost 1 in every 4 people.26 When looking at Tonga’s ability to combat its high prevalence of NCDs, the country scored 56 out of 100 in quality of healthcare, which was the 129th highest score out of 188 countries globally and 5th out of 12 countries in the Oceania region.27
Q: What areas within Tonga experience the highest risk for NCDs?
A: As mentioned earlier, urban areas in Tonga, such as within the city of Nuku’alofa, are at higher risk for NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7 than rural areas because they have greater access to imported goods that are high in energy and low in nutrition. In a study focused on maternal nutritional status, it was found that 72% of women living in the highest wealth quintile reported consuming foods made with oil, fat, and butter, in contrast to only 43.4% of women living in the lowest wealth quintile. The same trend was seen for sugary foods, with 59.2% of women in the highest wealth quintile reporting consumption in contrast to 37.4% of women in the lowest wealth quintile. A quintile is 1 of 5 equally divided groups, in this case, divided according to wealth status. Those of higher wealth status reside in urban areas, while those of lowest wealth status reside in rural areas.28 Areas where imported goods are more accessible results in a higher risk for NCDs because the poor quality of food consumption is the main risk factor for the development of NCDs.29 The poor quality of food consumption will be discussed in greater detail in the contributing factors section.

Q: What is malnutrition and how does it affect the people of Tonga?
A: The WHO gives daily energy intake recommendations to help prevent all forms of malnutrition and subsequent NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7.30 Malnutrition is defined as deficiencies, excesses, or imbalances in a person's intake of nutrients; it can exist in the form of both overnutrition and undernutrition.31 Due to the cultural and social prevalence of food and eating rituals among the people of Tonga, malnutrition presents itself most prevalently as overnutrition in this region.32 When there is a surplus of nutrients in the body, the body cannot utilize the excess energy and convert it into fat for later use. Sustained overconsumption patterns lead to unhealthy weight gain, which is one of the primary risk factors for developing NCDs.33 Unhealthy food and beverage consumption is recognized by the WHO as a significant contributor to the development of diabetesIncludes both type 1 and type 2 Diabetes Mellitus. Type 1 DM is different from type 2 in that it is an autoimmune disorder developed solely due to a person's genetics rather than lifestyle choices., heart disease, stroke, and cancer.34
Contributing Factors
Consumption
Food and Beverage Consumption
Due to the significant effect of food consumption on everyday body function, sustained poor diet choices among adults in Tonga steadily influence the development of NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7. The effect that diet has on the development of NCDs is commonly presented in conditions such as elevated blood pressure, blood glucose, and cholesterol levels, which are common contributors to the development of NCDs.35 General guidelines given by the World Health Organization emphasized the importance of consuming fruits and vegetables on a daily basis. Potatoes, sweet potatoes, cassava, and other starchy roots are excluded from this list because they readily break down into glucose, which increases blood sugar. Total energy intake from free sugarAll sugars added to foods or drinks by the manufacturer, cook, or consumer, as well as sugars naturally present in honey, syrups, fruit juices, and fruit juice concentrates.2 should ideally be less than 10%, energy intake from fats should be less than 30% with a preference towards unsaturated fats, and less than 5g of salt should be consumed per day.36
A study analyzing the energy and nutrient intake of Tongan adults observed that the average energy intake from fat is 32%, with the highest sources of fat intake including mutton (23%), chicken (10%), and coconut (10%).37 While this percentage is not alarmingly higher than the recommended (less than 30%), these fat sources are high in saturated fat. Saturated fat is a major contributor to increased blood cholesterol levels, which leads to an increase in ischemic heart diseaseA disease that develops due to a buildup of plaque on the walls of the heart arteries, which are responsible for supplying blood to the heart muscle. An excess of cholesterol in the blood commonly forms this plaque. This disease is also known as coronary heart disease (CHD) or coronary artery disease.5.38
Another aspect unique to energy consumption in Tonga is frequent feasting. Food is important for the maintenance of social relationships, which results in frequent large feasts called kaipola.39 In a study that analyzed Tongan’s energy and nutrient intakes over a period of 14 days, the mean energy intake was about 12.2 MJ (2,914 calories) for men and 10.6 MJ (2,532 calories) for women.40 During this time they were able to record 3 feast days and found that the mean daily energy intake on feast days was more than 20% higher than energy intake on non-feast days.41 Tongans participate in feasts on a regular basis as feasting commonly accompanies events such as weddings, funerals, state occasions, church conferences, and following church on the Sabbath.42 While there are no studies that measure the exact health implications of feasting, it is important to note that these periodic spikes of significant overconsumption well exceed the recommended range of calorie consumption for men (2000–3200 calories) and women (1600–2200 calories), based on individual factors such as age and activity levels.43 When calories are consumed in excess, they are stored within the body in the form of triglyceridesThe most common form of fat found in the body. They can come directly from high-fat foods, or are formed from excess consumption of calories.8. Over time, these triglycerides cause problems such as weight gain and buildup of plaque within the body's arteries, both of which are risk factors for the development of NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7 such as diabetesIncludes both type 1 and type 2 Diabetes Mellitus. Type 1 DM is different from type 2 in that it is an autoimmune disorder developed solely due to a person's genetics rather than lifestyle choices. and ischemic heart diseaseA disease that develops due to a buildup of plaque on the walls of the heart arteries, which are responsible for supplying blood to the heart muscle. An excess of cholesterol in the blood commonly forms this plaque. This disease is also known as coronary heart disease (CHD) or coronary artery disease.5.44
Tobacco and Alcohol Consumption
Tobacco and alcohol consumption is widely recognized as major contributors to NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7, as they threaten the normal function of the body's vital organs.45 The primary form of tobacco use in Tonga is smoking.46 As smoke-contaminated air is ultimately delivered throughout the entire body, harmful chemicals begin to damage the heart and blood vessels.47 There are over 7,000 different chemicals found in tobacco smoke, 250 of which are known to be harmful and 69 of which are known to cause cancer.48 Smoking tobacco is a common risk factor for the development of many NCDs, including CVD, diabetesIncludes both type 1 and type 2 Diabetes Mellitus. Type 1 DM is different from type 2 in that it is an autoimmune disorder developed solely due to a person's genetics rather than lifestyle choices., cancers, and chronic respiratory disease.49 Due to its harmful effects and influence on the development of NCDs, the WHO estimates that tobacco kills up to half of its users worldwide.50 In 2021, Tonga’s country profile report indicated that 16.6% of women and 53.7% of men aged 15–49 were active consumers of tobacco.51 Furthermore, it was measured that tobacco use among women peaked around ages 25–34, which coincides with peak childbearing years.52 Women in Tonga who are actively using tobacco during pregnancy are increasing their risk for lung damage and depriving their bodies of fresh, plentiful amounts of oxygen to support their vital organs and blood vessels. Continuous deprivation of fresh oxygen not only increases the risk for the development of NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7 but increases the risk of having a small or low-birth-weight baby.53 Low birth weight is regarded by the World Health Organization as an antecedent to NCDs developed later in life.54
Similarly to tobacco, alcohol consumption is harmful to the body and is strongly linked to cancer, cardiovascular disease, liver disease, pancreatitis, and diabetesIncludes both type 1 and type 2 Diabetes Mellitus. Type 1 DM is different from type 2 in that it is an autoimmune disorder developed solely due to a person's genetics rather than lifestyle choices..55 As alcohol is readily absorbed throughout the body, its effects take place on a cellular level, disrupting and weakening normal cell function. As certain cells throughout the body are affected by alcohol, they present a plethora of problems to virtually every body organ, namely the heart, liver, brain, and pancreas.56 According to the most recent STEPS report, 14.7% of Tongan men aged 18–69 were current drinkers (those who consumed alcohol in the past 30 days) compared to 5.3% of women in the same age group. Combined, only 8.7% of adults reported being current drinkers.57 While regular alcohol consumption is less of a concern in Tonga than tobacco consumption, heavy drinking remains a viable concern. With adults having reported drinking an average of 2.7 times within the last 30 days, 5.2% of respondents reported consuming 6 or more drinks in a single drinking occasion over that same time period. This consumption means that almost 60% of current drinkers engage in heavy drinking behaviors multiple times a month.58 As alcohol is consumed in such large quantities, it is more likely for the body to suffer damage to its vital organs.59 The WHO claims that harmful alcohol consumption causes more than 10% of the burden of NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7 globally, including cirrhosis of the liver, pancreatitis, oral, pharynx, larynx, esophagus, liver, and colorectal cancers, stroke, and hypertension.60
Sedentary Living
Sedentary behaviors lead to non-communicable diseasesA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7 because the body must expend excess energy input in order to maintain physiological homeostasisThe tendency towards a relatively stable equilibrium between interdependent elements, especially maintained by physiological processes.4, which is the body’s ability to achieve a relatively stable equilibrium between and within its 11 interdependent systems.61 Such sustained strain on the body as energy intake chronically exceeds energy outputs causes the body to develop NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7 over time.
In this process, scientific evidence widely supports that sedentary behaviors lead to an increase in overweight and obesityA disease primarily characterized by an excessive amount of body fat. It is most frequently determined by a measurement of weight that is considered too high compared to a person's height..62 Obesity plays a significant role in the development of other NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7 and has been found to be the single most prominent risk factor in the development of T2DMA chronic condition characterized by excess sugar in the bloodstream. Decreased pancreatic and cellular functions decrease the body’s ability to utilize glucose as a primary energy source. Left untreated, it can lead to severe malfunctions of the primary body systems.9 and CVD.63 In 2016, 75.6% of Tonga’s population was recognized as being overweight or obese, the 8th highest rate in the world.64 Modest weight loss and regular physical activity has been seen to prevent or delay T2DM by up to 58% in people with pre-diabetes.65 In 2012 it was measured that almost 1 in every 4 Tongans aged 24–64 did not engage in adequate amounts of physical activity.66

Obesity among women is of much greater concern than obesity among men, with the overall range of population prevalence at 67.2–76.3% for women and 49.4–60.7% for men.67 While it is clear that sedentary behaviors play a significant role in the prevalence of obesityA disease primarily characterized by an excessive amount of body fat. It is most frequently determined by a measurement of weight that is considered too high compared to a person's height., it is difficult to determine how much can be attributed to sedentary living itself. For instance, a Finnish diabetesIncludes both type 1 and type 2 Diabetes Mellitus. Type 1 DM is different from type 2 in that it is an autoimmune disorder developed solely due to a person's genetics rather than lifestyle choices. prevention study found that while increasing physical activity is important in preventing diabetes, it is primarily the resulting weight reduction that is most beneficial to preventing and reducing the occurrence of T2DMA chronic condition characterized by excess sugar in the bloodstream. Decreased pancreatic and cellular functions decrease the body’s ability to utilize glucose as a primary energy source. Left untreated, it can lead to severe malfunctions of the primary body systems.9.68 However, because obesity itself is classified as an NCD, sedentary living and the resulting lack of exercise can still be viewed as contributing factors for NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7 in Tonga.
Genetic Predisposition and Familial Culture
As genetics can account for large differences in the prevalence of diseases between populations, it is an important factor to consider when determining the risk of NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7 in Tonga. The thrifty gene hypothesis, first proposed by James V. Neel in 1962, suggests that Tongans began to develop genes that promote high fat and energy storage because of the adverse environments they historically faced. As Tongans engaged in long voyages across the ocean, they were forced to participate in periods of feasting and starvation as they were presented with limited opportunities to eat.69, 70 While the accuracy of this proposal has previously been unclear, data now suggests that a specific gene associated with increased body mass indexThe most common tool for determining obesity. Based on a person's weight and height, they are given a number; if a person’s BMI number reaches 30 or above, they are considered obese.1, the gene PPARGC1A, has been found to occur at a higher frequency among Polynesians. This data may help explain why Tonga sits at the 22nd highest prevalence of T2DMA chronic condition characterized by excess sugar in the bloodstream. Decreased pancreatic and cellular functions decrease the body’s ability to utilize glucose as a primary energy source. Left untreated, it can lead to severe malfunctions of the primary body systems.9 in the world.71, 72
Photo from Paul K on Flickr
When examining the occurrence of NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7 among families, it is common for clustering to occur.73 This clustering means that members of the same family have similar trends in the prevalence of NCDs and NCD risk factors. According to a study done in 2014, 50% of obesityA disease primarily characterized by an excessive amount of body fat. It is most frequently determined by a measurement of weight that is considered too high compared to a person's height. and T2DMA chronic condition characterized by excess sugar in the bloodstream. Decreased pancreatic and cellular functions decrease the body’s ability to utilize glucose as a primary energy source. Left untreated, it can lead to severe malfunctions of the primary body systems.9 cases with levels significantly different than the average occurrence could be explained by familial ties.74 While it is still difficult to determine if NCDs among Tongan adults are a product of genetics or not, it is clear that significant risk factors are closely associated with genetics.75
Risk factors for NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7, such as high cholesterol and high blood pressure, are likely to be inherited and then made worse by a combination of outside factors such as poor food consumption, tobacco and alcohol consumption, and sedentary behavior. In many cases, genes that predispose a person to diseases such as cancer or diabetesIncludes both type 1 and type 2 Diabetes Mellitus. Type 1 DM is different from type 2 in that it is an autoimmune disorder developed solely due to a person's genetics rather than lifestyle choices. are passed from parent to child and then triggered by various environmental factors. If a parent possesses a faulty gene, their offspring has a 50% chance of acquiring it. The likelihood of this gene contributing to the development of disease varies as it depends largely on the environment.76, 77 As NCDs remain difficult for adults to manage, children subsequently follow adult behavioral and environmental patterns, thus propelling the cycle of NCDs within families.78 An analysis of the food consumption patterns among children in Ha’apai, Tonga, it was found that children are following the same trends as adults and transitioning away from a traditional diet, instead consuming imported goods that are energy dense and poor in nutrients. The obesogenic environment that is heavily supported by the daily decisions of the country’s adult population is driving up childhood obesityA disease primarily characterized by an excessive amount of body fat. It is most frequently determined by a measurement of weight that is considered too high compared to a person's height. rates and is proving to be detrimental to childhood health and the risk for NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7.79 Childhood drug and alcohol consumption is also a major concern according to the 2017 Global School-Based Health Survey in Tonga. The report states that 14.5% of children aged 13–17 are current alcohol drinkers, 9.1% have used marijuana at least once in their lifetime, and 17.7% are current tobacco users.80 ‘Current’ consumers were defined as those who had consumed the product at least once within the last 30 days. It is significant to note that 37.5% of students reported that their parents or guardians use tobacco.81 This same report gathered data on physical activity and found that 24.8% of students reported not being physically active for at least 60 minutes on any day during the past 7 days.82 Since the cause of NCDs is a complex interplay between social, economic, and cultural factors, these genetic factors combined with NCD-contributing lifestyle choices are likely to increase the prevalence of NCDs among future generations.83 Further research into genetic predisposition would help in determining what mix of other factors should be focused on in order to reduce the instance of NCDs among adults in Tonga.
Consequences
Morbidity and Mortality
The prevalence of NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7 is a significant driver of morbidityGeneral disease or suffering that occurs because of a medical condition. and mortalityRefers to death or the state of being subject to death. rates due to the adverse effects that NCDs have on the body. For instance, one case of morbidity that occurs in Tonga is limb amputation due to T2DMA chronic condition characterized by excess sugar in the bloodstream. Decreased pancreatic and cellular functions decrease the body’s ability to utilize glucose as a primary energy source. Left untreated, it can lead to severe malfunctions of the primary body systems.9. Common complications of T2DM include poor blood circulation and nerve damage. These complications increase a person’s likelihood of developing an ulcer, which worsens quickly under the circumstances and causes damage to the tissues and bones, leading to a need to amputate.84 One study in Tonga found that 272 out of 4,653 diabetesIncludes both type 1 and type 2 Diabetes Mellitus. Type 1 DM is different from type 2 in that it is an autoimmune disorder developed solely due to a person's genetics rather than lifestyle choices. patients from 2004–2012 received lower limb amputations.85 Another source estimates that about 41 major amputations take place in Tonga every year.86 The amputation of a limb brings the need for ongoing care to individuals who neglected to access sufficient healthcare in the first place. As diabetic amputations are associated with an increased risk of subsequent death, diabetic amputations in Tonga significantly contribute to a decreased quality of life.87 As amputations continue to make up a significant portion of overall morbidityGeneral disease or suffering that occurs because of a medical condition. in Tonga, the overall quality of life will decrease.
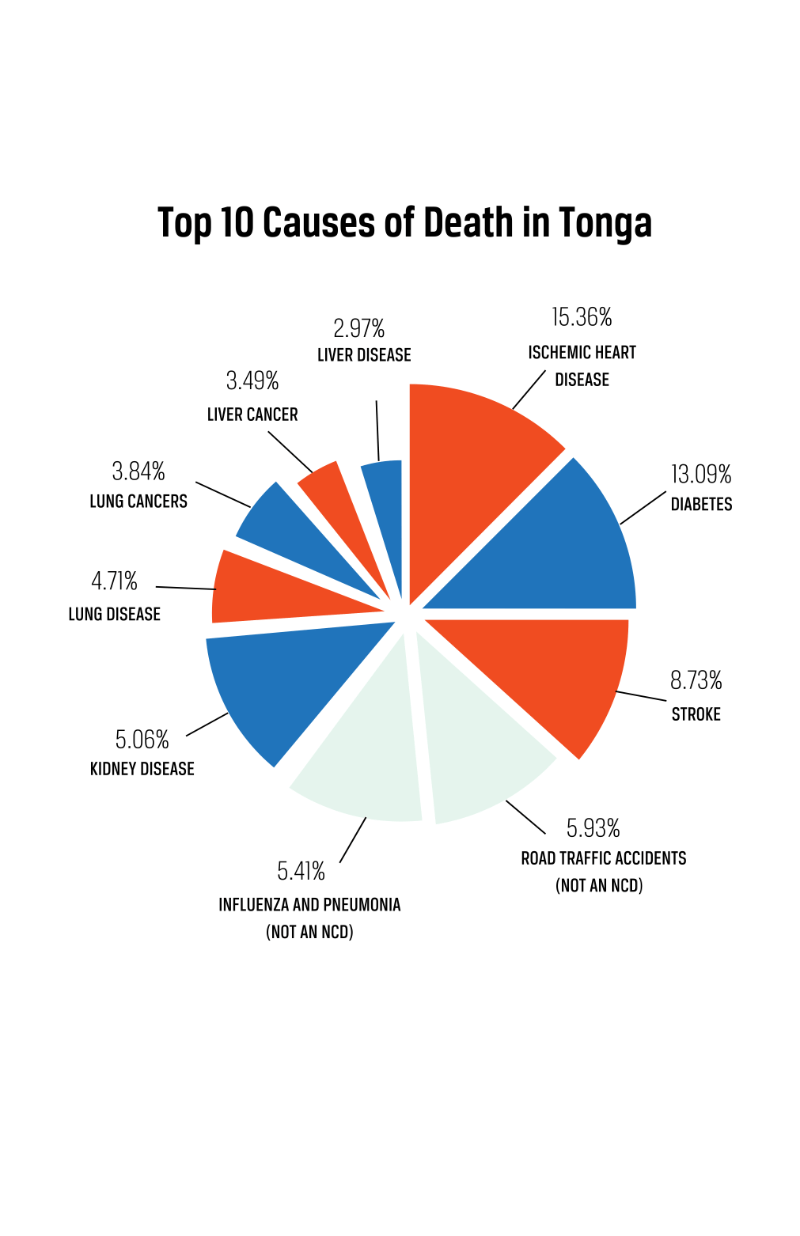
NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7 claim responsibility for 83% of deaths in Tonga, with a 23% probability of these deaths occurring prematurely.88 As of 2022, the top 3 leading causes of death in Tonga include ischemic heart diseaseA disease that develops due to a buildup of plaque on the walls of the heart arteries, which are responsible for supplying blood to the heart muscle. An excess of cholesterol in the blood commonly forms this plaque. This disease is also known as coronary heart disease (CHD) or coronary artery disease.5, diabetesIncludes both type 1 and type 2 Diabetes Mellitus. Type 1 DM is different from type 2 in that it is an autoimmune disorder developed solely due to a person's genetics rather than lifestyle choices., and stroke—all of which are NCDs. Out of the top 10 causes of death, all but 2 are NCDs.89 It is also significant to acknowledge the interrelated nature of NCDs in deciphering the significance of NCDs’ role in mortalityRefers to death or the state of being subject to death. rates. A study that analyzed the National Diabetes Registry along with the National Deaths Registry in Tonga found that diabetes mellitusIncludes both type 1 and type 2 Diabetes Mellitus. Type 1 DM is different from type 2 in that it is an autoimmune disorder developed solely due to a person's genetics rather than lifestyle choices. was a contributing factor in 50% of deaths due to sepsis, 57.1% of deaths due to kidney failure, 43.8% of deaths due to stroke, and 33.9% of deaths due to ischaemic heart disease.90 This data confirms that the presence of an NCD is a risk factor for developing an additional NCD. As an individual continues to develop NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7 and therefore develops risk factors for further development of additional NCDs, their quality of life will decrease as they experience higher levels of personal morbidityGeneral disease or suffering that occurs because of a medical condition..
Increased Government, Economic, and Healthcare Burden
Because NCD treatment demands significant financial, healthcare, and human resources, NCD prevalence in Tonga leads to an increased burden on the government, economic well-being, and the healthcare system. According to the World Bank, the global cost of NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7 in Gross Domestic Profit (GDP) is about 3.25%.91 This number is much higher in Tonga, where the cost of NCDs is about 8.3% of the GDP.92 Based on the current growth of NCDs within the country, this number is expected to increase to 12.3% by 2040.93 Furthermore, the country is projected to have lost 18.5% of its effective labor force by the same time.94 It is estimated that 23% of NCD-related deaths occur prematurely (below the age of 60) in Tonga.95 Globally, people aged 15–64 are considered to be part of the working age group,96 meaning that the working population that serves to maintain economic stability in Tonga is significantly impacted by NCD prevalence.97 NCDs also have a negative impact on worker productivity. Both a decrease in the available workforce and decreased labor productivity are directly linked to a decrease in GDP.98
Unlike many other countries around the world, Tonga’s government funds the vast majority of healthcare costs in the country. In a study conducted in 2019, health expenditure in Tonga had taken up 11–15% of total government budgets over the previous 5 years.99 Of the total amount of money spent within the country on health care, 84% of the money came directly from the government.100 While this health system protects Tongan citizens from poverty or financial strain due to health expenses, it places a growing financial burden on government health budgets which cannot be sustained with the rising rates of NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7.101 Due to a variety of unique geographical and economic barriers, rapid economic growth is highly unlikely to be achieved, meaning that long-term care and maintenance of NCDs cannot be financially sustained.102 It is important to note that NCDs are incurable, chronic diseases that require medical attention over time. Symptoms can be treated through long-term medications, lifestyle modifications, and regular screening.103 The cost of treatment varies depending on each NCD and the treatment required. For example, the cost of treating an NCD can quickly become astronomical when dealing with a prognosis that includes chemotherapy or an organ transplant.
Practices
Pacific Legislative Framework for NCDs
The Pacific Legislative Framework (PLF) is an initiative published by the Public Health Division of the Pacific Community. The framework was designed by a collection of legislative drafters, legal officers, and health policy experts across the pacific region.103 The framework covers 21 Pacific Island countries and territories (PICTs), including Tonga, and was recently finalized in 2021 after a series of regional and individual PICT consultations beginning in March 2019. The framework is funded by the Commonwealth Secretariat, the Australian Department of Foreign Affairs and Trade, and the New Zealand Ministry of Foreign Affairs and Trade.104 The PLF was created to strengthen the use of legislative approaches across all sectors that address NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7 and NCD risk factors. It was created under the belief that the implementation of effective legislative measures is critical to addressing the growing burden of NCDs in the Pacific region.105
Through the Pacific Monitoring Alliance for NCD Action, an assessment of the effectiveness of current key regional strategies to address NCDs was performed. It was found that most PICTs need to strengthen their NCD-related laws and regulations in order to establish control over NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7.106 With this information, it was determined that a PLF for NCDs would significantly aid in reducing the prevalence of NCDs in the region. The PLF sets forth policies to address and prevent NCD risk factors such as alcohol consumption, tobacco control, regulation of marketing of unhealthy foods and beverages, and reducing consumption of salt, sugar, and trans-fat.107 The overall goal of the program is to enable PICTs across the Pacific region to work together in meeting the worldwide goal to reduce NCDs by one-third by 2030.108 The intended implementation of the PLF begins with the individual PICTs undertaking a gap analysis of their current NCD-related laws. Throughout this process, they are to critically analyze and compare their current legislation with the PLF, identify any weaknesses, propose any amendments, and produce a policy document on the review of NCD-related legislation.109 This policy document should then be presented to and approved by the government. Following approval, new bills or amendments to current bills can be made.110 The PLF contains sample drafts of bills and regulations to help the PICT through this process. For each risk factor to be addressed, the PLF lays out legislative policies, legislative plans, and draft legislative provisions.111 PICTs are expected to follow the recommendations within each component in order to create and establish reformed policies that better protect their country against NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7.112
Impact
Impact data on the PLF is not yet available due to the youth of the program. However, it is important to note that based on their research, the WHO recognizes legislative policies as an effective and essential method of reducing this number, and this brief will demonstrate the efficacy of legislative policies to combat NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7 using data from legislation preceding the PLF, including legislation from other countries.113 Measuring the impact of NCD interventions is similar to measuring NCD prevalence in that the focus is primarily on NCD risk factors. Support for NCD prevention legislative policies is grounded in the success of policies such as smoking bans in public places. In a study of 12 countries (including Turkey, USA, Canada, Australia, New Zealand, Hong Kong, Argentina, Panama, and Uruguay), it was found that there was a significant association between decreased risk of cardiovascular problems and the implementation of smoking bans.114 More specifically to Tonga, a 2019 publication showed that implemented policies surrounding taxation have also been successful within Tonga. Research showed that around 76–79% of smokers reported smoking less because of price changes. Increased taxation was also reported by 98–99% of people as the reason they had cut back on mutton flapA cut of meat from a lamb's breast known for its relatively low cost and high-fat content.6 consumption.115
One of the tools that are used in the Pacific to monitor NCD interventions is the Pacific Monitoring Alliance for NCD Action (MANA) tool. It uses a ‘traffic light’ rating scheme to track the progress of 21 different Pacific Island Countries and Territories (PICT) over time. A red indicator shows no policy or action present, an amber indicator shows a policy or action under development, and a green indicator shows a policy or action in place. Once an indicator is green, the strength of the policy or action is shown using a star system. A policy can have anywhere between 0–3 stars, 3 being the strongest policy or action. Comparing the baseline report in Tonga from 2017–2018 to the most recent report from 2019–2020, we can see that the alcohol taxation policy increased in strength from 0 to 2 stars. Preventative policies reducing salt consumption moved from red to one star, trans-fats moved from red to yellow, and implementing healthy food policies within schools moved from yellow to 3 stars. It is important to note that these measurements were taken before the PLF was officially finalized. The improvement seen here can be attributed to the regional strategies which are taken into consideration and improved within the PLF.
Gaps
While the PLF is an intervention that covers a wide variety of factors that could reduce the occurrence of NCDsA health condition that is non-transmissible and non-infectious. It is typically long-lasting and developed over time due to genetic, lifestyle, environmental, or physiological factors.7 across the PICTs, it lacks efficient and specific methods of measurement. Because the framework has put forth recommendations that are applicable to 21 different PICTs, it is difficult to measure how well its recommendations apply to the various peoples and cultures within the specific PICTs. In Tonga, the PLF lacks unique strategies that are catered specifically to the Tongan people. For example, the main focuses of the PLF surrounding tobacco control include: regulating the tobacco industry’s role in interfering with public health policies, increasing the use of graphic health warnings, especially on tobacco packaging, controlling tobacco sales and licensing, and raising tobacco taxes. While addressing these factors would likely work well if the main form of tobacco consumption came from local manufacturers and tobacco imported from foreign industries, it lacks the understanding that the majority of smokers in Tonga smoke Tapaka Tonga, the locally grown, untaxed, and hand-rolled tobacco.116
The MANA system, originally created in 2017 to measure the effectiveness of regional NCD strategies throughout the pacific, is likely one of the tools that will be used to indirectly measure the PLF’s influence in Tonga. Even though the MANA tool measures such a wide variety of NCD indicators, the traffic light system offers little insight as to what improvements under each category have been made. A green indicator may be representative of an implemented policy that barely touches the real problem, as in the case of the recommendations surrounding tobacco control. While the PLF identifies negative consequences that exist because of the problem, death, disability, reduced productivity, and burden on governments, communities, and families, it does not provide any information that indicates whether or not this intervention is helping to improve those consequences within the specific PICTs.117 The framework also disregards the reality of the contributing factors that extend beyond the scope of legislation, such as genetics, culture, and lifestyle choices.
Preferred Citation: Vaitohi, Autumn. “Prevalence of Non-Communicable Disease among Adults in Tonga.” Ballard Brief. December 2022. www.ballardbrief.byu.edu.
Viewpoints published by Ballard Brief are not necessarily endorsed by BYU or The Church of Jesus Christ of Latter-day Saints