
Presence of Malnutrition and Severe Acute Malnutrition among Children in South Asia


By Madison Johnson
Published Fall 2022
Special thanks to Robyn Mortensen for editing and research contributions.
Summary+
South Asia is home to 23% of the global population and has the largest prevalence of stunting in any region in the world. Severe acute malnutrition is a frequent cause of death in children under 5 globally. 1 While sustainable development goals have brought more people out of poverty in the last 50 years, a disproportionate number of children remain malnourished. These children are typically found in developing countries, with a large burden existing in South Asia. Young children are most susceptible to the effects of malnutrition as they are at a stage of increased physical and cognitive development. There are many contributors to this problem in South Asia: mainly due to inflating food prices, lack of education, and other familial or living conditions. Many of the physical and cognitive effects children suffer under the age of 5 due to malnutrition are irreversible after age 5 and can lead to death or severe disability. Government groups are standardizing the method of identifying and treating severe acute malnutrition in children, and some groups are implementing those methods; however, the impact needs to be more rigorously studied to show how implementing best practices affect the outcomes of malnourished individuals.
Key Takeaways+
- Malnutrition poses a high mortality risk for children, with nearly half of all deaths of children under 5 being related to SAM.
- Gender, age, family size, living conditions, food inflation, and inadequate education all lead to an increase in childhood malnutrition.
- Children not only suffer from physical difficulties due to malnutrition but also cognitive deficiencies and poor quality of life.
- Interventions via screening, educating, and nurturing children early in childhood have proven to help alleviate malnutrition; however, there is a lack of homogeneity between organizations focusing on the same issue.
- The Bountiful Children’s Foundation’s intervention model has aspects proven to alleviate child malnutrition and break the cycle of malnutrition and proves that interventions can be cost-effective.
Key Terms+
Acute malnutrition—A nutritional deficiency resulting from either inadequate energy or protein intake. The presence of wasting (being underweight), though less common than chronic malnutrition, carries a higher risk of mortality.2
Anemia—A deficiency of hemoglobin or red cells in the blood. The most common form of anemia is iron deficiency anemia. Children who suffer from anemia are often stunted. Pregnant women who suffer from anemia are at higher risk of having low-weight babies. Around 42% of children under 5 and 40% of pregnant women globally are estimated to suffer from anemia.3
Chronic malnutrition—The most common form of malnutrition and causes stunting (short individuals). It is an irreversible condition after 2 years of age.4
Diet-related Non-Communicable diseases (NCDs)—Unhealthy diet and nutrition are driving the increase of non-communicable diseases such as diabetes and cardiovascular disease. Overly processed and cheap foods are the main source of poor diets among poorer populations. Other NCDs that have been attributed to diet are stroke and some cancers.5
Disability Affected Life Years (DALYs)—One DALY represents the loss of the equivalent of one year of full health. DALYs for a disease or health condition are the sum of the years of life lost due to premature mortality (YLLs) and the years lived with a disability (YLDs) due to prevalent cases of the disease or health condition in a population.6
Double Burden of Malnutrition—The coexistence of undernutrition along with obesity and being overweight, diet-related non-communicable diseases within individuals, households, and populations.7
Food insecurity—A temporary or long-term condition characterized by inadequate access to sufficient foods necessary for health. This can result due to insufficient income or access to nutrient-dense foods.
Intergenerational Cycle of Malnutrition—The intergenerational cycle is the path through which a low-birth-weight baby becomes a stunted child, a stunted adolescent, and a malnourished woman who, in turn, has another low-birth-weight baby.8
Malnutrition—Malnutrition refers to deficiencies, excesses, or imbalances in a person’s intake of energy or nutrients. The term malnutrition covers 2 broad groups of conditions. One is undernutrition—which includes stunting (low height for age), wasting (low weight for height), underweight (low weight for age), and micronutrient deficiencies or insufficiencies (a lack of important vitamins and minerals). The other is overweight, obesity, and diet-related non-communicable diseases (such as heart disease, stroke, diabetes, and cancer).9
SAM—Severe acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%).
South Asia—While the South Asian region’s countries may differ by source and may or may not include countries in Southeast Asia as well, for the purpose of this brief, we will refer to the entire region as South Asia, with the following countries being included:
The countries in South and Southeast Asia are Afghanistan, Bangladesh, Bhutan, India, Iran, Maldives, Nepal, Pakistan, and Sri Lanka. Southeast Asian countries include Brunei, Cambodia, Indonesia, Laos, Malaysia, Myanmar, Philippines, Singapore, Thailand, Timor-Leste, and Vietnam.
Stunting—A condition where someone is too short for their height, signaling poor nutritional health in the stages of growth, especially for children. A child that is 2 standard deviations below the mean height growth for their age will be identified as stunted.
Wasting—A comparison of a child’s weight compared to their height. Wasting signals that a child has had recent or severe weight loss. This happens from poor nutrition or frequent illness.10
Context
Q: What is severe acute malnutrition, and what are its risk factors in South Asia?
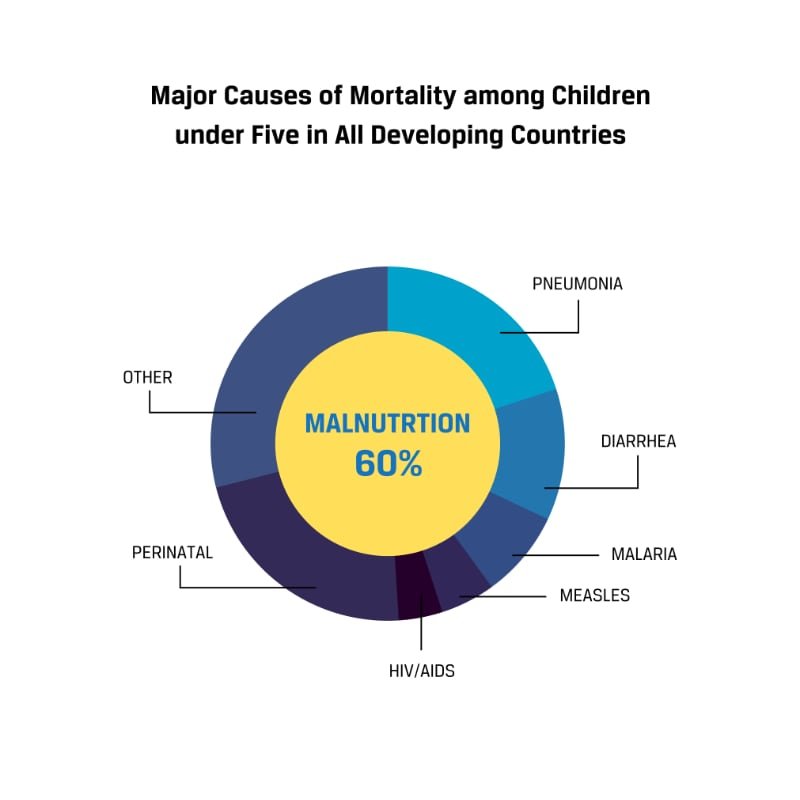
A: Severe acute malnutritionSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%). (SAM) is a condition of extreme malnourishment that can be life-threatening for young children. SAM occurs when children are very low weight for their height (known as wasting) and very short for their age (known as stunting). General malnutritionMalnutrition refers to deficiencies, excesses, or imbalances in a person’s intake of energy or nutrients. The term malnutrition covers 2 broad groups of conditions. One is undernutrition—which includes stunting (low height for age), wasting (low weight for height), underweight (low weight for age), and micronutrient deficiencies or insufficiencies (a lack of important vitamins and minerals). The other is overweight, obesity, and diet-related non-communicable diseases (such as heart disease, stroke, diabetes, and cancer).9 can refer to people on both ends of the nutritional spectrum—either overweight or underweight.11 Malnutrition holds a high level of mortality risk in children under 5. Malnutrition is linked (as a comorbidity) to 45% of child deaths under 5. Eleven and a half percent of deaths in children under 5 are attributable solely to acute malnutritionA nutritional deficiency resulting from either inadequate energy or protein intake. The presence of wasting (being underweight), though less common than chronic malnutrition, carries a higher risk of mortality.2, with 7.8% attributable to SAM.12 Poor maternal health, improper breastfeeding, and poor nutrition under age 5, among other things, are risk factors for developing SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%). in the region. Not breastfeeding exclusively for 6 months and lack of proper food intake after 6 months are the main risk factors for SAM in children.

While SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%). is a very complex issue, it is important to understand the difference between the prevalence and the burden of malnutritionMalnutrition refers to deficiencies, excesses, or imbalances in a person’s intake of energy or nutrients. The term malnutrition covers 2 broad groups of conditions. One is undernutrition—which includes stunting (low height for age), wasting (low weight for height), underweight (low weight for age), and micronutrient deficiencies or insufficiencies (a lack of important vitamins and minerals). The other is overweight, obesity, and diet-related non-communicable diseases (such as heart disease, stroke, diabetes, and cancer).9. Some children may suffer from SAM for an extended period of time, while others may experience frequent episodes, and others may only experience SAM for a short period. What many sources show is the prevalence of malnutrition, not accounting for the true number of people who suffer from malnutrition globally each year. To explain this, K-factor was invented to show that while the prevalence of malnutritionMalnutrition refers to deficiencies, excesses, or imbalances in a person’s intake of energy or nutrients. The term malnutrition covers 2 broad groups of conditions. One is undernutrition—which includes stunting (low height for age), wasting (low weight for height), underweight (low weight for age), and micronutrient deficiencies or insufficiencies (a lack of important vitamins and minerals). The other is overweight, obesity, and diet-related non-communicable diseases (such as heart disease, stroke, diabetes, and cancer).9 may be one number, the burden may be 6–9 times higher. K-factor is a correction coefficient that compares the burden of malnutrition (often very high) to the prevalence (what most sources use to estimate malnutrition). “Of the estimated 47 million children under 5 with acute malnutritionA nutritional deficiency resulting from either inadequate energy or protein intake. The presence of wasting (being underweight), though less common than chronic malnutrition, carries a higher risk of mortality.2 in 2019, 14 million suffered from severe acute malnutritionSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%). and 33 million from moderate acute malnutrition. When we apply the corresponding K-factors (6 and 5, respectively) to these prevalence numbers—with the caveat that these are based solely on data from West African children under 2 years old—we find that, in fact, up to 295 million children likely experienced acute malnutritionA nutritional deficiency resulting from either inadequate energy or protein intake. The presence of wasting (being underweight), though less common than chronic malnutrition, carries a higher risk of mortality.2 in 2019.”13 These numbers are from West Africa, but if we applied the K-factor model to the severity of SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%). in South AsiaWhile the South Asian region’s countries may differ by source and may or may not include countries in Southeast Asia as well, for the purpose of this brief, we will refer to the entire region as South Asia, with the following countries being included: The countries in South and Southeast Asia are Afghanistan, Bangladesh, Bhutan, India, Iran, Maldives, Nepal, Pakistan, and Sri Lanka. Southeast Asian countries include Brunei, Cambodia, Indonesia, Laos, Malaysia, Myanmar, Philippines, Singapore, Thailand, Timor-Leste, and Vietnam., we would find that malnutritionMalnutrition refers to deficiencies, excesses, or imbalances in a person’s intake of energy or nutrients. The term malnutrition covers 2 broad groups of conditions. One is undernutrition—which includes stunting (low height for age), wasting (low weight for height), underweight (low weight for age), and micronutrient deficiencies or insufficiencies (a lack of important vitamins and minerals). The other is overweight, obesity, and diet-related non-communicable diseases (such as heart disease, stroke, diabetes, and cancer).9 is a larger issue that affects even more people than most sources say.
Q: What is the double burden?
A: The double burden occurs when someone is both malnourished and overweight. The double burden of malnutritionThe coexistence of undernutrition along with obesity and being overweight, diet-related non-communicable diseases within individuals, households, and populations.7 has only recently become a problem due to changes in gene expression due to generational malnutritionMalnutrition refers to deficiencies, excesses, or imbalances in a person’s intake of energy or nutrients. The term malnutrition covers 2 broad groups of conditions. One is undernutrition—which includes stunting (low height for age), wasting (low weight for height), underweight (low weight for age), and micronutrient deficiencies or insufficiencies (a lack of important vitamins and minerals). The other is overweight, obesity, and diet-related non-communicable diseases (such as heart disease, stroke, diabetes, and cancer).9. This change in gene expression happens on a cellular level when a child suffers from SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%).. When a child is malnourished, the gene expression of their children changes. While DNA is unaffected, the expression of their genes does change. This change is manifest in insulin resistance, unexplained weight gain, and other weight-related issues.14 This cellular change leads to other nutrition-related illnesses like abnormal blood sugar and fatty liver disease, which can lead to rapid weight loss or weight gain. When a child suffers from these metabolic illnesses, it increases the genetic risk of passing these illnesses to their children.15
Q: Who is most affected by SAM?
A: Children are the most commonly affected by improper nutrition—especially children under the age of 5, those who live in poverty, in large families, and whose parents are less educated or illiterate.16 While different cultures affect whether or not boys or girls are affected more by malnutritionMalnutrition refers to deficiencies, excesses, or imbalances in a person’s intake of energy or nutrients. The term malnutrition covers 2 broad groups of conditions. One is undernutrition—which includes stunting (low height for age), wasting (low weight for height), underweight (low weight for age), and micronutrient deficiencies or insufficiencies (a lack of important vitamins and minerals). The other is overweight, obesity, and diet-related non-communicable diseases (such as heart disease, stroke, diabetes, and cancer).9, what we see is that females are disproportionately affected by the double burden of malnutritionThe coexistence of undernutrition along with obesity and being overweight, diet-related non-communicable diseases within individuals, households, and populations.7. The double burden occurs when someone is both undernourished and overweight.17 While males generally need more calories than females, females need more specific nutrients such as iron and folic acid. The difference in nutrient needs makes it harder for females to avoid SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%). while eating the same types of food as their male counterparts.18 It is estimated that women and girls make up 60% of those suffering from food insecurityA temporary or long-term condition characterized by inadequate access to sufficient foods necessary for health. This can result due to insufficient income or access to nutrient-dense foods. in the world.19 Many mothers who experienced SAM as children develop anemiaA deficiency of hemoglobin or red cells in the blood. The most common form of anemia is iron deficiency anemia. Children who suffer from anemia are often stunted. Pregnant women who suffer from anemia are at higher risk of having low-weight babies. Around 42% of children under 5 and 40% of pregnant women globally are estimated to suffer from anemia.3 as adults, which is a leading cause of maternal death worldwide.20
Being female does not cause malnutrition, but if a boy and a girl are undernourished equally, the girl is more likely to develop malnutrition because she requires additional nutrients to be healthy. While females, in general, need fewer calories than males, they need more calcium, folate, and iron than males in order to remain healthy and grow properly. Females have higher nutrient needs to have adequate reproductive health long term. Adequate amounts of these minerals are particularly difficult to get from diet alone during pregnancy, exacerbating the deficits from lack of health care and improper diet that often exist in low-income countries.21, 22 Other effects may influence the disproportionate effect of females suffering from SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%). as well, such as male preference in certain cultures leading to societal and economic bias against women.23
Q: When did this issue start, and how has it changed over time?
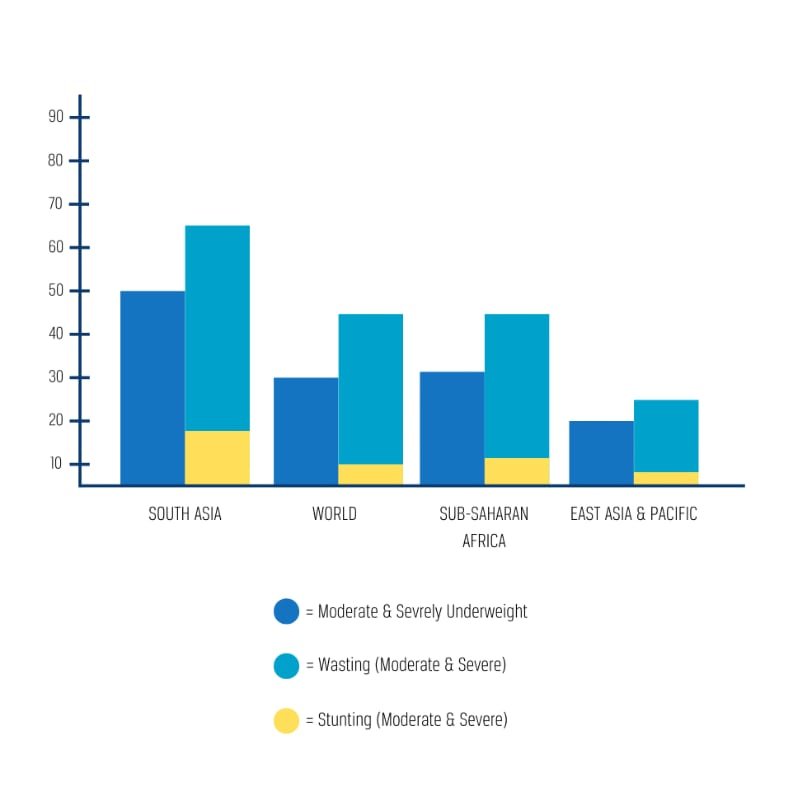
A: Asia has more than half of the world’s stunted children, more than two-thirds of all wasted children, and almost half of overweight children. While the prevalence of stuntingA condition where someone is too short for their height, signaling poor nutritional health in the stages of growth, especially for children. A child that is 2 standard deviations below the mean height growth for their age will be identified as stunted. has decreased for some of the countries in South AsiaWhile the South Asian region’s countries may differ by source and may or may not include countries in Southeast Asia as well, for the purpose of this brief, we will refer to the entire region as South Asia, with the following countries being included: The countries in South and Southeast Asia are Afghanistan, Bangladesh, Bhutan, India, Iran, Maldives, Nepal, Pakistan, and Sri Lanka. Southeast Asian countries include Brunei, Cambodia, Indonesia, Laos, Malaysia, Myanmar, Philippines, Singapore, Thailand, Timor-Leste, and Vietnam. over the past 30 years, other countries in the region have seen little to no change.24 South Asia as a whole has seen a decrease in 2 decades from 61% prevalence of stunting to 38%.25 In Thailand, wastingA comparison of a child’s weight compared to their height. Wasting signals that a child has had recent or severe weight loss. This happens from poor nutrition or frequent illness.10 increased from 5% to 7% prevalence for children between 2006–2012.
The UN Agencies estimate that the undernourished population in Asia as a whole increased from 361.3 million to 418.0 million between 2019–2020, which increased the prevalence of undernourishment from 7.9% to 9.0%.26 South Asia had the most severe impact, accounting for 89% of the increase in the number of undernourished in Asia.27
Globally, 144 million children under 5 are stunted, with a higher prevalence in low-income families.28 In recent years, the number of people living in extreme poverty in South AsiaWhile the South Asian region’s countries may differ by source and may or may not include countries in Southeast Asia as well, for the purpose of this brief, we will refer to the entire region as South Asia, with the following countries being included: The countries in South and Southeast Asia are Afghanistan, Bangladesh, Bhutan, India, Iran, Maldives, Nepal, Pakistan, and Sri Lanka. Southeast Asian countries include Brunei, Cambodia, Indonesia, Laos, Malaysia, Myanmar, Philippines, Singapore, Thailand, Timor-Leste, and Vietnam. has gone down; however, it is estimated that an additional 4.7 million people were pushed into extreme poverty due to the COVID-19 pandemic.29 Because more families have been pushed into extreme poverty, there is an increased likelihood of children developing SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%). in those households due to the intertwined nature of SAM and poverty. In Myanmar, 111,000 children are expected to become wasted as a direct result of the pandemic.30 This issue has affected all low-income countries during developmental stages and is perpetual in countries unable to break through the development stage. Despite global efforts to combat this issue, malnutritionMalnutrition refers to deficiencies, excesses, or imbalances in a person’s intake of energy or nutrients. The term malnutrition covers 2 broad groups of conditions. One is undernutrition—which includes stunting (low height for age), wasting (low weight for height), underweight (low weight for age), and micronutrient deficiencies or insufficiencies (a lack of important vitamins and minerals). The other is overweight, obesity, and diet-related non-communicable diseases (such as heart disease, stroke, diabetes, and cancer).9 is still considered to be the #1 global health threat by the World Health Organization (the governing body of global health) because it affects more people than any other health threat.31
Q: How does SAM in South Asia compare to other regions of the world?
A: The South AsiaWhile the South Asian region’s countries may differ by source and may or may not include countries in Southeast Asia as well, for the purpose of this brief, we will refer to the entire region as South Asia, with the following countries being included: The countries in South and Southeast Asia are Afghanistan, Bangladesh, Bhutan, India, Iran, Maldives, Nepal, Pakistan, and Sri Lanka. Southeast Asian countries include Brunei, Cambodia, Indonesia, Laos, Malaysia, Myanmar, Philippines, Singapore, Thailand, Timor-Leste, and Vietnam. region shows signs of being the highest region affected by childhood malnutritionMalnutrition refers to deficiencies, excesses, or imbalances in a person’s intake of energy or nutrients. The term malnutrition covers 2 broad groups of conditions. One is undernutrition—which includes stunting (low height for age), wasting (low weight for height), underweight (low weight for age), and micronutrient deficiencies or insufficiencies (a lack of important vitamins and minerals). The other is overweight, obesity, and diet-related non-communicable diseases (such as heart disease, stroke, diabetes, and cancer).9 in the world.32 Within Asia, rates of SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%). are significantly higher in South Asian countries, with more than half of the global number of children suffering from SAM residing in 5 countries: Afghanistan, Bangladesh, India, Indonesia, and Pakistan.33 Although the number of undernourished people was higher in sub-Saharan Africa, the presence of child malnutrition was much higher in Southern Asia.34, 35 For example, in Cambodia and Indonesia, 32% and 31% (respectively) of all children experience chronic malnutritionThe most common form of malnutrition and causes stunting (short individuals). It is an irreversible condition after 2 years of age.4, which manifests as stuntingA condition where someone is too short for their height, signaling poor nutritional health in the stages of growth, especially for children. A child that is 2 standard deviations below the mean height growth for their age will be identified as stunted..36, 37, 38 While 22% of children globally under 5 suffer from stunting, South Asia has a higher prevalence of stunting.39 Additionally, South Asia has seen a large increase in the “double burden” of malnutrition in recent years.40
Q: How is SAM identified and treated?
A: The process of identifying and treating SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%). is fairly standardized globally. SAM is identified based on a child’s nutritional status. Children can be identified as being at risk of developing malnutritionMalnutrition refers to deficiencies, excesses, or imbalances in a person’s intake of energy or nutrients. The term malnutrition covers 2 broad groups of conditions. One is undernutrition—which includes stunting (low height for age), wasting (low weight for height), underweight (low weight for age), and micronutrient deficiencies or insufficiencies (a lack of important vitamins and minerals). The other is overweight, obesity, and diet-related non-communicable diseases (such as heart disease, stroke, diabetes, and cancer).9 if previous siblings or their parents have suffered from malnutrition or by looking at their recent food intake and determining if there has been recent weight or height loss in the child.41 Two main tests exist to determine the current nutritional status of children: measurement of upper arm circumference and the height and weight of a child compared to normal growth charts.42
Fortified milk, breastfeeding, supplements, or food variety may be used in situations where someone is suffering from SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%)..43 Many interventions exist, but most have a common focus on children in the first 1,000 days of life or pregnant and breastfeeding women.44, 45 Additional preventive measures focus on educating mothers on household nutrition as well as educating children in schools about health.46 Treatment programs for SAM will be more fully discussed in the practices section of this brief.

Contributing Factors
Generational Poverty
The vast majority of people suffering from SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%). reside in low to middle-income countries.47 Children from larger households have poorer diets and have a greater risk of stuntingA condition where someone is too short for their height, signaling poor nutritional health in the stages of growth, especially for children. A child that is 2 standard deviations below the mean height growth for their age will be identified as stunted. even when adjusted for economic status.48 Like the cycle of poverty, malnutritionMalnutrition refers to deficiencies, excesses, or imbalances in a person’s intake of energy or nutrients. The term malnutrition covers 2 broad groups of conditions. One is undernutrition—which includes stunting (low height for age), wasting (low weight for height), underweight (low weight for age), and micronutrient deficiencies or insufficiencies (a lack of important vitamins and minerals). The other is overweight, obesity, and diet-related non-communicable diseases (such as heart disease, stroke, diabetes, and cancer).9 is linked to the cycle from generation to generation. Our understanding of poverty suggests that while people born into poverty tend to stay in poverty, there are deeper layers. Impoverished people tend to have less access to varieties of food necessary for proper growth. Growth retardation leads to decreased economic output and tends to keep people in poverty across generations.49

Extreme poverty creates a risk for children to develop SAM because it increases the difficulty for families to access nutrient-rich foods, decreases their buying power due to inflation, and limits the amount they can spend on education. Nearly all children identified with SAM live in low and middle-income countries.50 In most countries, nearly all children identified to be suffering from SAM come from the lowest sociodemographic groups within those countries.51 In South AsiaWhile the South Asian region’s countries may differ by source and may or may not include countries in Southeast Asia as well, for the purpose of this brief, we will refer to the entire region as South Asia, with the following countries being included: The countries in South and Southeast Asia are Afghanistan, Bangladesh, Bhutan, India, Iran, Maldives, Nepal, Pakistan, and Sri Lanka. Southeast Asian countries include Brunei, Cambodia, Indonesia, Laos, Malaysia, Myanmar, Philippines, Singapore, Thailand, Timor-Leste, and Vietnam., the poorest groups have the highest risk of developing SAM.52
Price Increase in Staple Foods
In addition to low income, the poorest households are at increased risk of developing SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%). as prices of staple foods inflate. Low-income households are more adversely affected by price increases in staple foods because they are unable to purchase a variety of nutrient-rich foods. Many of the most nutritious foods are also the most expensive, whereas highly-processed foods, which have a low nutritional value, are the cheapest and most accessible.53 In certain areas of South AsiaWhile the South Asian region’s countries may differ by source and may or may not include countries in Southeast Asia as well, for the purpose of this brief, we will refer to the entire region as South Asia, with the following countries being included: The countries in South and Southeast Asia are Afghanistan, Bangladesh, Bhutan, India, Iran, Maldives, Nepal, Pakistan, and Sri Lanka. Southeast Asian countries include Brunei, Cambodia, Indonesia, Laos, Malaysia, Myanmar, Philippines, Singapore, Thailand, Timor-Leste, and Vietnam., the prices of staple foods have increased and continue to increase. For example, global prices of wheat have increased by over 50% in the last year alone. Rice prices also are inflating.54, 55, 56, 57 Other staples, such as meat, have seen large inflation due to a number of factors, such as animal illnesses. The UN Food Price Index shows food prices have increased globally by 75% since the beginning of the pandemic.58 This is due to various factors such as rising demand, supply chain difficulty, import and export tariffs, crop failure, livestock sickness and death, and labor shortages. This affects the purchasing power of the money families have. When staple food prices increase, families buy less of the foods they regularly eat, decreasing the quantity of food they eat. Because people typically purchase their staple foods first each time they shop, as prices increase, other nutritious foods are bought less because the amount of money left over decreases. This leads to decreased quality of foods eaten.59 As more people are pushed into poverty due to inflation, we can reasonably expect that more people will suffer from SAM, and the generational effects will also be present, as we have seen in the past.
Education
Lack of adequate education for both parents is shown to be a leading predictor of SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%). in children. Many families cannot afford to send their children to school, or they need their children to work to supplement the family income.60 Nutritional education efforts start in formal school settings.61 There is a direct correlation between the educational status of a child's parents (especially the mother) and the nutritional status of her child, as seen in various studies.62, 63, 64
A review of recent studies in South AsiaWhile the South Asian region’s countries may differ by source and may or may not include countries in Southeast Asia as well, for the purpose of this brief, we will refer to the entire region as South Asia, with the following countries being included: The countries in South and Southeast Asia are Afghanistan, Bangladesh, Bhutan, India, Iran, Maldives, Nepal, Pakistan, and Sri Lanka. Southeast Asian countries include Brunei, Cambodia, Indonesia, Laos, Malaysia, Myanmar, Philippines, Singapore, Thailand, Timor-Leste, and Vietnam. shows that lack of education for parents is one of the leading factors of SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%). in young children and indicates that increasing education could lead to a decrease in SAM predictors.65, 66 In remote and rural areas, it is common for mothers to be illiterate or have less education.67 Low levels of primary education of mothers and rates of SAM in their children are highly correlated. Further, many people who are not able to have formal schooling stay in lower socioeconomic statuses—further exacerbating the risk of SAM.68, 69
Because of the cost of education, many families cannot afford to send their children to school. Rather they have their children work to supplement the family income. Household contribution to overall education expense in low and middle-income countries is 36%, over double the contribution made by households in high-income countries such as the US at 16%. This means that families incur a higher burden to send their kids to school in lower-income countries.70 Many families are not able to pay for educational expenses, especially when they have multiple children, because it accounts for a greater percentage of their income than in higher-income countries.71 As people are less educated, leading to long-term poverty, we see an increase in SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%)..72
Poor Prenatal Care, Breastfeeding, and Toddler Feeding Practices
Maternal Health and Breastfeeding
Poor nutritional status of a child can be linked to maternal nutrition and maternal health care before and during pregnancy. While there are many factors that increase the likelihood of SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%)., the effects of malnutritionMalnutrition refers to deficiencies, excesses, or imbalances in a person’s intake of energy or nutrients. The term malnutrition covers 2 broad groups of conditions. One is undernutrition—which includes stunting (low height for age), wasting (low weight for height), underweight (low weight for age), and micronutrient deficiencies or insufficiencies (a lack of important vitamins and minerals). The other is overweight, obesity, and diet-related non-communicable diseases (such as heart disease, stroke, diabetes, and cancer).9 on children start in the embryo, when mothers are inadequately nourished. A mother’s lack of nutrition while pregnant increases the likelihood of SAM more than any other factor.73 This leads to children who are more likely to be born with low birth weight, are stunted in their growth from inception, and are at risk for premature birth.74, 75
Whether children are born at a healthy weight or underweight, we find that breastfeeding practices impact growth as well. Growth faltering usually begins between 3–6 months of a child’s life and is connected to the mother ceasing to breastfeed.76 Growth faltering is also associated with mothers who do not initiate early breastfeeding (within one hour of birth).77 In Indonesia and the Philippines, exclusive breastfeeding before 6 months was practiced by less than 40% of women; in Vietnam, the rate was as low as 15.5%.78
While exclusive breastfeeding is an important practice for the first 6 months of a child’s life, after 6 months, exclusive breastfeeding can be harmful. If children are only exclusively breastfed, they see detriments to their growth as breastmilk alone does not provide adequate nutrition for children of that age group.79 The likely main reason that people have improper breastfeeding practices is that they are not educated on the matter. One study shows that in South AsiaWhile the South Asian region’s countries may differ by source and may or may not include countries in Southeast Asia as well, for the purpose of this brief, we will refer to the entire region as South Asia, with the following countries being included: The countries in South and Southeast Asia are Afghanistan, Bangladesh, Bhutan, India, Iran, Maldives, Nepal, Pakistan, and Sri Lanka. Southeast Asian countries include Brunei, Cambodia, Indonesia, Laos, Malaysia, Myanmar, Philippines, Singapore, Thailand, Timor-Leste, and Vietnam. as well as sub-Saharan Africa, 74.7–89.9% of women in the lowest two wealth quintiles (who are also generally less educated) reported giving birth at home.80 When women have children at home and without proper midwife care, it is unlikely that they will already know about proper breastfeeding practices.
After babies are born, improper breastfeeding practices lead to an increased risk of malnutritionMalnutrition refers to deficiencies, excesses, or imbalances in a person’s intake of energy or nutrients. The term malnutrition covers 2 broad groups of conditions. One is undernutrition—which includes stunting (low height for age), wasting (low weight for height), underweight (low weight for age), and micronutrient deficiencies or insufficiencies (a lack of important vitamins and minerals). The other is overweight, obesity, and diet-related non-communicable diseases (such as heart disease, stroke, diabetes, and cancer).9 in children under 24 months because children do not get the nutrients necessary for proper growth. Breastmilk has many necessary micronutrients, such as iron, Vitamin A, zinc, and iodine which are necessary for proper growth in infants. Improper breastfeeding practices may include not breastfeeding at all, not exclusively breastfeeding for the first 6 months, or not breastfeeding immediately after birth.81
Toddler Feeding Practices
When children are no longer breastfeeding age (after 24 months old), lack of dietary diversity is one of the main causes of SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%)..82 Other reasons they are affected are a lack of safe food and eating practices and poor complementarity (breastfeeding and solid foods together) in foods that are necessary for growth. It has been found that proper growth for children is most likely to be achieved if the child is introduced to foods supplemental to breastfeeding at around 6 months and then increases the number of solid foods to wean off breastfeeding over time.83 If food is introduced too early (before 6 months), children may develop infections, and breastfeeding may end prematurely. In one study, it was found that 70% of South Asian women began weaning children off of breastfeeding at 3 months (which is much earlier than guidelines suggest).84 Only about 52% of children 6–8 months old are breastfed and simultaneously fed solid foods in South AsiaWhile the South Asian region’s countries may differ by source and may or may not include countries in Southeast Asia as well, for the purpose of this brief, we will refer to the entire region as South Asia, with the following countries being included: The countries in South and Southeast Asia are Afghanistan, Bangladesh, Bhutan, India, Iran, Maldives, Nepal, Pakistan, and Sri Lanka. Southeast Asian countries include Brunei, Cambodia, Indonesia, Laos, Malaysia, Myanmar, Philippines, Singapore, Thailand, Timor-Leste, and Vietnam..85 Young children also require more frequent feedings of small meals because of their limited gastric capacity. Limited diversity and low frequency of feeding are linked to SAM in children under age 2. In South Asia, the diversity of food is more commonly a problem than the frequency of feeding.86
Poor Sanitation, Hygiene, and Living Conditions
The existence of harmful bacteria in water sources increases the likelihood of suffering from bacterial illness and increases mortality when coupled with SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%).. While clean living conditions alone do not guarantee a healthy child, unclean living conditions may exacerbate symptoms of SAM. Bacterial illnesses are directly linked with poor nutrient absorption and SAM.87 Poor sanitation also carries an increased risk of foodborne illnesses. Additionally, sanitation is a prerequisite to healthy digestion and the absence of harmful parasites. Diarrhea, for example, is a bacterial disease that shows a person is under digesting their food.88, 89 Proper hygiene (handwashing, not defecating openly, drinking clean water, etc.) is also important to keep children from bringing harmful bacteria into living spaces and developing other diseases that perpetuate SAM. Bacterial illnesses have been shown to contribute to the development of SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%). and also increase the difficulty of eliminating SAM.90 South AsiaWhile the South Asian region’s countries may differ by source and may or may not include countries in Southeast Asia as well, for the purpose of this brief, we will refer to the entire region as South Asia, with the following countries being included: The countries in South and Southeast Asia are Afghanistan, Bangladesh, Bhutan, India, Iran, Maldives, Nepal, Pakistan, and Sri Lanka. Southeast Asian countries include Brunei, Cambodia, Indonesia, Laos, Malaysia, Myanmar, Philippines, Singapore, Thailand, Timor-Leste, and Vietnam. is one of the regions with the poorest sanitation and clean water in the world with 68–84% of its water sources being contaminated.91 Additionally, South Asia has the majority of the world’s open defecators.92
The average household size in Southeast Asia is roughly 4.5 people, with Laos being the country in the region with the highest household size (5.6).93 Comparatively, in the US and other developed countries, the average is about 2.6 people per household.94 Household size has been linked to SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%). because children who are born into larger families receive less nutrient-dense foods when there are limited food supplies, especially in poor households.95 Living in close proximity and in unsanitary conditions with lots of people can lead to the contraction of various bacterial diseases such as HIV, which is a common comorbidity for children with SAM.96 While poor sanitation practices themselves do not cause SAM in children, bad hygiene contributes to higher rates of SAM and comorbidities such as bacterial illness that have high mortality rates in children.97
Consequences
High Infant Mortality
SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%). is the leading cause of child mortality globally, with 45% of child deaths being linked to undernutrition.98 Children may die directly from SAM or from comorbidities such as infections that come as a result of suffering from SAM. A child experiencing wastingA comparison of a child’s weight compared to their height. Wasting signals that a child has had recent or severe weight loss. This happens from poor nutrition or frequent illness.10 in a low-income country is 12 times more likely to die than a healthy child in a high-income country.99 Because wasting in South AsiaWhile the South Asian region’s countries may differ by source and may or may not include countries in Southeast Asia as well, for the purpose of this brief, we will refer to the entire region as South Asia, with the following countries being included: The countries in South and Southeast Asia are Afghanistan, Bangladesh, Bhutan, India, Iran, Maldives, Nepal, Pakistan, and Sri Lanka. Southeast Asian countries include Brunei, Cambodia, Indonesia, Laos, Malaysia, Myanmar, Philippines, Singapore, Thailand, Timor-Leste, and Vietnam. affects over 250,000 children, SAM-related mortality is a major problem for the region. However, while SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%). on its own can lead to death, the main concern is that SAM leads to other deadly complications that largely do not exist among healthy children. Infections and disease are common comorbidities for children suffering from SAM.100 Younger children are disproportionately affected by poor diet because they need a higher ratio of nutrients to weight than older children and adults due to the rapid growth that occurs at a young age.101 For example, in Nepal, relative to 24–59-month-old children, children 6–12 months and 12–23 months had 12.1 and 6.6 (respectively) times higher odds of being severely malnourished, which also carries an increased risk of mortality.102 This means that the youngest children are those who are most at risk of dying due to SAM-related complications in South Asia.
In South AsiaWhile the South Asian region’s countries may differ by source and may or may not include countries in Southeast Asia as well, for the purpose of this brief, we will refer to the entire region as South Asia, with the following countries being included: The countries in South and Southeast Asia are Afghanistan, Bangladesh, Bhutan, India, Iran, Maldives, Nepal, Pakistan, and Sri Lanka. Southeast Asian countries include Brunei, Cambodia, Indonesia, Laos, Malaysia, Myanmar, Philippines, Singapore, Thailand, Timor-Leste, and Vietnam., the age where death is highest for children suffering from SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%). is up to 23 months. All people are susceptible to malnutritionMalnutrition refers to deficiencies, excesses, or imbalances in a person’s intake of energy or nutrients. The term malnutrition covers 2 broad groups of conditions. One is undernutrition—which includes stunting (low height for age), wasting (low weight for height), underweight (low weight for age), and micronutrient deficiencies or insufficiencies (a lack of important vitamins and minerals). The other is overweight, obesity, and diet-related non-communicable diseases (such as heart disease, stroke, diabetes, and cancer).9, but because younger children have underdeveloped immune systems and require greater amounts of nutrients, they are at a much higher risk of death when suffering from SAM.103 Malnutrition is the main contributor to disease susceptibility in children. It leads to underdeveloped immune and digestive systems that lead to an increased risk of developing deadly diseases such as autoimmune diseases, diarrheal illness, and respiratory infections.105, 105, 106
Irreversible Cognitive and Physical Deficiencies
When children under 5 do not receive sufficient interventions to treat malnutritionMalnutrition refers to deficiencies, excesses, or imbalances in a person’s intake of energy or nutrients. The term malnutrition covers 2 broad groups of conditions. One is undernutrition—which includes stunting (low height for age), wasting (low weight for height), underweight (low weight for age), and micronutrient deficiencies or insufficiencies (a lack of important vitamins and minerals). The other is overweight, obesity, and diet-related non-communicable diseases (such as heart disease, stroke, diabetes, and cancer).9, their brains do not develop properly, and the effects are irreversible.107 For an underdeveloped brain, some of the cognitive deficiencies that may arise are poor mental development, behavioral issues, and low scholastic achievement.108 Cognitive impairment and other physical illnesses can also shorten life span as well as decrease energy and ability to function into adulthood when a child is malnourished.109 The first 1,000 days of life are attributed to be the time when the majority of cognitive development occurs. When a child at this age experiences malnutrition, the cognitive effects can be catastrophic. Individuals who are malnourished only as adults are spared the cognitive effects of malnutrition, whereas children are affected heavily.110, 111, 112
Physical deficiencies also occur to the level of becoming irreversible when children are not nourished in those first 1,000 days. Disability Affected Life YearsOne DALY represents the loss of the equivalent of one year of full health. DALYs for a disease or health condition are the sum of the years of life lost due to premature mortality (YLLs) and the years lived with a disability (YLDs) due to prevalent cases of the disease or health condition in a population.6 (DALY’s), or the shortened lifespan for a disabled person, increases when a child suffers from malnutritionMalnutrition refers to deficiencies, excesses, or imbalances in a person’s intake of energy or nutrients. The term malnutrition covers 2 broad groups of conditions. One is undernutrition—which includes stunting (low height for age), wasting (low weight for height), underweight (low weight for age), and micronutrient deficiencies or insufficiencies (a lack of important vitamins and minerals). The other is overweight, obesity, and diet-related non-communicable diseases (such as heart disease, stroke, diabetes, and cancer).9. While these physical effects do not immediately lead to death, they do lead to a decreased quality and length of life. Trillions of dollars lost can be attributed to the decrease in productivity and energy in workers who suffered from malnutrition as children and who continue to suffer from it into adulthood.113, 114 Micronutrient and amino acid deficiencies lead to underdevelopment on the cellular level in the brain. Those effects are largely irreversible. Adults who were malnourished in infancy and childhood have a lower capacity for energy storage and usage, decreasing their ability for activity and work and decreasing their expected life span.115 Life expectancy in 6 of 11 countries in South Asia is below the world average life expectancy of 73 years, with Afghanistan being the lowest at 65 years.116
StuntingA condition where someone is too short for their height, signaling poor nutritional health in the stages of growth, especially for children. A child that is 2 standard deviations below the mean height growth for their age will be identified as stunted. from malnutritionMalnutrition refers to deficiencies, excesses, or imbalances in a person’s intake of energy or nutrients. The term malnutrition covers 2 broad groups of conditions. One is undernutrition—which includes stunting (low height for age), wasting (low weight for height), underweight (low weight for age), and micronutrient deficiencies or insufficiencies (a lack of important vitamins and minerals). The other is overweight, obesity, and diet-related non-communicable diseases (such as heart disease, stroke, diabetes, and cancer).9 after 2 years of age can be permanent, irreversible, and fatal because it is directly linked to chronic illnesses that decrease life expectancy; South AsiaWhile the South Asian region’s countries may differ by source and may or may not include countries in Southeast Asia as well, for the purpose of this brief, we will refer to the entire region as South Asia, with the following countries being included: The countries in South and Southeast Asia are Afghanistan, Bangladesh, Bhutan, India, Iran, Maldives, Nepal, Pakistan, and Sri Lanka. Southeast Asian countries include Brunei, Cambodia, Indonesia, Laos, Malaysia, Myanmar, Philippines, Singapore, Thailand, Timor-Leste, and Vietnam. has the highest rate of stuntingA condition where someone is too short for their height, signaling poor nutritional health in the stages of growth, especially for children. A child that is 2 standard deviations below the mean height growth for their age will be identified as stunted. of any region in the world at 48% of the population.117. 118 Unlike failing to gain weight before age 5, stunting and height loss are largely irreversible.119 In cases where children continue to live after severe stunting and wastingA comparison of a child’s weight compared to their height. Wasting signals that a child has had recent or severe weight loss. This happens from poor nutrition or frequent illness.10 under age 5, their brains are never able to fully develop, and their immune systems are permanently compromised, leading to increased contraction of acute and chronic disease after age 5 and into adulthood.120 Diseases affecting the liver, heart, brain, pancreas, eyes, and gastrointestinal tract can be traced to child undernutrition in many developing countries.121
Behavioral problems are also linked to cognitive underdevelopment and malnutritionMalnutrition refers to deficiencies, excesses, or imbalances in a person’s intake of energy or nutrients. The term malnutrition covers 2 broad groups of conditions. One is undernutrition—which includes stunting (low height for age), wasting (low weight for height), underweight (low weight for age), and micronutrient deficiencies or insufficiencies (a lack of important vitamins and minerals). The other is overweight, obesity, and diet-related non-communicable diseases (such as heart disease, stroke, diabetes, and cancer).9. Those effects often continue into adulthood and cause further difficulty for already struggling people. When compared to non-stunted children, children who were stunted in early childhood were more likely to be hyperactive or have anxiety or depression.122 Undernutrition is also linked to an increase in the stress hormone cortisol.123 High cortisol levels are linked to chronic adult diseases in children who suffer from malnutrition. We also see increases in diabetes as well as weight gain later in life linked to these high cortisol levels.124 Verbal and spatial ability, as well as IQ, are directly affected when children under 5 are malnourished. Malnutrition is also linked to poor cognition in children.125
Intergenerational Malnutrition and Disability
If children live past infancy and are able to have children in the future, the effect of one’s childhood nutritional status will affect their offspring in future years. The largest deficit is seen in the generation immediately following a child with severe nutritional deficiencies, but effects are estimated to be seen in part for up to 12 generations later.126 Nutritional deficits in childhood affect an important part of DNA creation called methylation. This phenomenon is why in South AsiaWhile the South Asian region’s countries may differ by source and may or may not include countries in Southeast Asia as well, for the purpose of this brief, we will refer to the entire region as South Asia, with the following countries being included: The countries in South and Southeast Asia are Afghanistan, Bangladesh, Bhutan, India, Iran, Maldives, Nepal, Pakistan, and Sri Lanka. Southeast Asian countries include Brunei, Cambodia, Indonesia, Laos, Malaysia, Myanmar, Philippines, Singapore, Thailand, Timor-Leste, and Vietnam., we see stunted children being born to stunted parents (whose stuntingA condition where someone is too short for their height, signaling poor nutritional health in the stages of growth, especially for children. A child that is 2 standard deviations below the mean height growth for their age will be identified as stunted. began as children when methylation was taking place).127, 128 Part of the difficulty seen with intergenerational malnutritionMalnutrition refers to deficiencies, excesses, or imbalances in a person’s intake of energy or nutrients. The term malnutrition covers 2 broad groups of conditions. One is undernutrition—which includes stunting (low height for age), wasting (low weight for height), underweight (low weight for age), and micronutrient deficiencies or insufficiencies (a lack of important vitamins and minerals). The other is overweight, obesity, and diet-related non-communicable diseases (such as heart disease, stroke, diabetes, and cancer).9 is in the development of the reproductive system. Reproductive development can be affected as early as the embryo, causing a deficit in future generations. Maternal weight gain in childhood is positively associated with the better nutritional status of future children. Many deficiencies are programmed genetically in utero and cannot be reversed after birth. In addition to improper childhood nutrition, improper prenatal nutrition leads to many deficits in her children.129

Children who suffer from SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%). are more likely to have children who suffer from SAM or other disabilities. For mothers who were undernourished as girls, it is 40% more likely that their children do not live to age 5. They are also more likely to die during childbirth.130 SAM creates an intergenerational cycle of malnutritionThe intergenerational cycle is the path through which a low-birth-weight baby becomes a stunted child, a stunted adolescent, and a malnourished woman who, in turn, has another low-birth-weight baby.8 because children who suffer from SAM are more likely to have children who are malnourished. This is manifested in various ways—through stuntingA condition where someone is too short for their height, signaling poor nutritional health in the stages of growth, especially for children. A child that is 2 standard deviations below the mean height growth for their age will be identified as stunted., anemiaA deficiency of hemoglobin or red cells in the blood. The most common form of anemia is iron deficiency anemia. Children who suffer from anemia are often stunted. Pregnant women who suffer from anemia are at higher risk of having low-weight babies. Around 42% of children under 5 and 40% of pregnant women globally are estimated to suffer from anemia.3, and the double burden of malnutritionThe coexistence of undernutrition along with obesity and being overweight, diet-related non-communicable diseases within individuals, households, and populations.7 (presence of stunting and overweight). A mother who is underweight or anemic is more likely to have a child who is stunted.131 Roughly 1 in 3 women of maternal age is anemic globally. Nearly 40% of children between 6 months–5 years of age suffer from anemia.132 In Southeast Asia, over 50% of women of reproductive age suffer from anemia.133 Anemia causes there to be less oxygen in the blood, and if left untreated, it can damage the heart and cause issues during pregnancy.134 Anemia before or during pregnancy is the main risk factor for having a preterm or underweight baby. There is also an increased risk of death when a mother gives birth due to complications that occur more frequently, such as excessive bleeding after birth.135, 136 When mothers have underweight babies, those children start life at a disadvantage and will need more intervention than children who are born at a normal weight. When children suffer from anemiaA deficiency of hemoglobin or red cells in the blood. The most common form of anemia is iron deficiency anemia. Children who suffer from anemia are often stunted. Pregnant women who suffer from anemia are at higher risk of having low-weight babies. Around 42% of children under 5 and 40% of pregnant women globally are estimated to suffer from anemia.3, there are a number of symptoms, including fatigue, gastrointestinal problems, and trouble with concentration and memory. Anemia can cause further complications by making children more susceptible to diseases and infections.137 Children will oftentimes appear pale and weak when suffering from anemia, similar to how they would appear when suffering from SAM.138 There is a strong link between child anemia and SAM.139, 140
There is a strong correlation between child malnutritionMalnutrition refers to deficiencies, excesses, or imbalances in a person’s intake of energy or nutrients. The term malnutrition covers 2 broad groups of conditions. One is undernutrition—which includes stunting (low height for age), wasting (low weight for height), underweight (low weight for age), and micronutrient deficiencies or insufficiencies (a lack of important vitamins and minerals). The other is overweight, obesity, and diet-related non-communicable diseases (such as heart disease, stroke, diabetes, and cancer).9 and maternal anemiaA deficiency of hemoglobin or red cells in the blood. The most common form of anemia is iron deficiency anemia. Children who suffer from anemia are often stunted. Pregnant women who suffer from anemia are at higher risk of having low-weight babies. Around 42% of children under 5 and 40% of pregnant women globally are estimated to suffer from anemia.3. Anemia, like malnutrition, has intergenerational consequences.141 Even when children of previously malnourished parents are not malnourished themselves, there is a higher prevalence of disorders such as ADD and OCD.142 Malnutrition leads to a change in how genes behave, causing deficits for generations after one is malnourished. In these cases, reversibility is only possible with rigorous healthcare interventions.143 Childhood malnutrition, when untreated, leads to negative impacts on genetic metabolism for life.144 When there is no intervention before age 5, the effects are largely irreversible. If children under 5 are malnourished, it can lead to intergenerational malnutrition or disability. Of the roughly half a million maternal deaths at birth, over half occur in South AsiaWhile the South Asian region’s countries may differ by source and may or may not include countries in Southeast Asia as well, for the purpose of this brief, we will refer to the entire region as South Asia, with the following countries being included: The countries in South and Southeast Asia are Afghanistan, Bangladesh, Bhutan, India, Iran, Maldives, Nepal, Pakistan, and Sri Lanka. Southeast Asian countries include Brunei, Cambodia, Indonesia, Laos, Malaysia, Myanmar, Philippines, Singapore, Thailand, Timor-Leste, and Vietnam..145 Additionally, nearly half of low birthweight babies occur in the same region.146 Low birth weight for girls is correlated with SAM in their children, making child malnutrition an intergenerational issue.147, 148
Practices
The Bountiful Children’s Foundation is a social problem-solving organization (SPSO) that focuses on eliminating malnutritionMalnutrition refers to deficiencies, excesses, or imbalances in a person’s intake of energy or nutrients. The term malnutrition covers 2 broad groups of conditions. One is undernutrition—which includes stunting (low height for age), wasting (low weight for height), underweight (low weight for age), and micronutrient deficiencies or insufficiencies (a lack of important vitamins and minerals). The other is overweight, obesity, and diet-related non-communicable diseases (such as heart disease, stroke, diabetes, and cancer).9, specifically in a child’s first 1,000 days of life. A child’s brain grows the most during this time.149 Adequate or lack of nutrition lays the foundation for the lifelong growth potential of children.150 After correctly identifying those with SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%)., Bountiful works towards eliminating malnutrition through education and nutrition. They help pregnant women with prenatal care, provide nutritional supplements for lactating mothers and their children, provide nutritional education for parents, and distribute local nutrient-rich foods and supplements so that families learn which foods they should eat.

Bountiful uses the World Health Organization’s methods to identify children suffering from SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%).. They use height, weight, and arm circumference tests in conjunction. This is done by measuring a child’s weight and height in comparison to average healthy child growth charts. Those identified as being a certain standard deviation below the mean growth weight and height are considered to have severe acute malnutritionSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%). (SAM). The upper arm circumference test is used to detect underweight children and the protein and fat content of their bodies. At birth, head circumference is also an effective tool to determine where a child is at, but as they grow older, it is less predictive of SAM.151
Bountiful has programs in 20 countries currently, with Cambodia and the Philippines included in their South AsiaWhile the South Asian region’s countries may differ by source and may or may not include countries in Southeast Asia as well, for the purpose of this brief, we will refer to the entire region as South Asia, with the following countries being included: The countries in South and Southeast Asia are Afghanistan, Bangladesh, Bhutan, India, Iran, Maldives, Nepal, Pakistan, and Sri Lanka. Southeast Asian countries include Brunei, Cambodia, Indonesia, Laos, Malaysia, Myanmar, Philippines, Singapore, Thailand, Timor-Leste, and Vietnam. program. Access to supplements, food, and other resources like nutritional education is linked to the prevention and treatment of SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%).. Interventions vary depending on the severity of the malnutritionMalnutrition refers to deficiencies, excesses, or imbalances in a person’s intake of energy or nutrients. The term malnutrition covers 2 broad groups of conditions. One is undernutrition—which includes stunting (low height for age), wasting (low weight for height), underweight (low weight for age), and micronutrient deficiencies or insufficiencies (a lack of important vitamins and minerals). The other is overweight, obesity, and diet-related non-communicable diseases (such as heart disease, stroke, diabetes, and cancer).9 and the age of the child. The focus of Bountiful is to get children adequate nutrition to keep them healthy until the age of 5, when they are more apt to fend off diseases. Bountiful also helps families understand the importance of proper hygiene, sanitation, and clean water and gives them access to resources that help prevent SAM.152
Bountiful addresses these issues by providing supplements for both children and pregnant or lactating mothers. Throughout childhood, Bountiful also monitors growth every six months to measure the child’s progress. Additionally, Bountiful provides classes and materials about hygiene, healthy food preparation, and meal planning. It costs the organization $8.00 per month to feed a child the necessary vitamins and minerals for proper growth.
Bountiful has outlined its practices very thoroughly; however, there is room for improvement when measuring the effectiveness of the intervention. For example, they mention specific outputs such as the number of children reached, the number of screenings conducted, the number of provided supplements, and the number of health lessons taught. What we do not know is how much of a change these interventions are having on individuals. A comparison of children before and after the intervention, as well as a comparison of non-participants, would give us a better understanding of the effectiveness of this group. Additional measurements, such as health lessons, effectiveness in isolation, and supplemental effect in isolation, will also show which aspects of the program have the greatest impact. From speaking with their employees, it was learned that these measurements do take place but are not listed on the website. The recommendation would be that they include these measurements to show a more holistic impact the organization is having on individual lives.
Looking at the global impact that’s been made by many SPSOs working toward ending SAMSevere acute malnutrition. Unlike generalized malnutrition, this refers to undernutrition explicitly. Covers undernutrition (specifically the bottom 5%)., from 2000–2020, the percentage of children globally who were stunted decreased by roughly 11%, while the global population has increased by 28%.153 The percentages of wastingA comparison of a child’s weight compared to their height. Wasting signals that a child has had recent or severe weight loss. This happens from poor nutrition or frequent illness.10, underweight, and stunted children have declined from 3.5%, 4.5%, and 8.9% to 1.7%, 3.3%, and 5.0%, respectively, showing that interventions like Bountiful are proven to be effective.154
Preferred Citation: Johnson, Madison. “Presence of Malnutrition and Severe Acute Malnutrition Among Children in South Asia.” Ballard Brief. December 2022. www.ballardbrief.byu.edu.
Viewpoints published by Ballard Brief are not necessarily endorsed by BYU or The Church of Jesus Christ of Latter-day Saints